Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Your Doctor Is A Liar! CHOLESTEROL DOES NOT CAUSE HEART DISEASE!Document566 pagesYour Doctor Is A Liar! CHOLESTEROL DOES NOT CAUSE HEART DISEASE!greensmokee276100% (14)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Comprehensive Cardiovascular Medicine in The Primary Care Setting-Humana Press (2018) PDFDocument530 pagesComprehensive Cardiovascular Medicine in The Primary Care Setting-Humana Press (2018) PDFHaribabu ArumugamPas encore d'évaluation
- Edexcel IAL Biology Unit 1 Topic 1 - Molecules, Transport and HealthDocument40 pagesEdexcel IAL Biology Unit 1 Topic 1 - Molecules, Transport and HealthEshalPas encore d'évaluation
- The Ultimate Liver CleanseDocument26 pagesThe Ultimate Liver CleanseBradford S. Weeks100% (8)
- Cardiovascular ImagingDocument401 pagesCardiovascular ImagingRani Mulia100% (5)
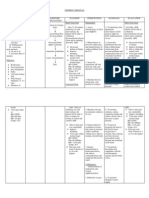
- NURSING CARE PLAN For Myocardial InfarctionDocument13 pagesNURSING CARE PLAN For Myocardial Infarctionbanyenye2593% (14)
- Filipino Widow's Medical CaseDocument30 pagesFilipino Widow's Medical Casereginebenedicte100% (1)
- Toxic Oil Why Vegetable Oil Will Kill You and How To Save YourselfDocument260 pagesToxic Oil Why Vegetable Oil Will Kill You and How To Save YourselfKovaci Radu Florin100% (1)
- ABG analysis for respiratory failure therapy effectivenessDocument25 pagesABG analysis for respiratory failure therapy effectivenessHan Nah0% (1)
- Understanding Blood Vessels and HypertensionDocument99 pagesUnderstanding Blood Vessels and HypertensionGeorge Hanania100% (1)
- Framingham Risk Score SaDocument8 pagesFramingham Risk Score Saapi-301624030Pas encore d'évaluation
- AtherosclerosisDocument14 pagesAtherosclerosisDeepak Raj100% (1)
- General - Pathology 2Document15 pagesGeneral - Pathology 2ahmed jarad100% (2)
- Acute Biologic CrisisDocument60 pagesAcute Biologic Crisisraidis100% (4)
- Major MineralsDocument31 pagesMajor MineralsmissirenaPas encore d'évaluation
- DMS. K22. Obat TopikalDocument23 pagesDMS. K22. Obat TopikalmissirenaPas encore d'évaluation
- Fungal Infections of the Skin, Hair and NailsDocument120 pagesFungal Infections of the Skin, Hair and NailsmissirenaPas encore d'évaluation
- K1 - Histo Skin 2013Document36 pagesK1 - Histo Skin 2013Desi Indah LaisPas encore d'évaluation
- DMS. K15a. Connective Tissue DiseasesDocument37 pagesDMS. K15a. Connective Tissue DiseasesmissirenaPas encore d'évaluation
- K19 - Pharmacology of NAPZAededDocument62 pagesK19 - Pharmacology of NAPZAededwlmhfpPas encore d'évaluation
- DMS. K13. Antifungal + AntilepraDocument37 pagesDMS. K13. Antifungal + AntilepramissirenaPas encore d'évaluation
- Dms. k24. Skin Manifestations of Nutritional DisordersDocument33 pagesDms. k24. Skin Manifestations of Nutritional DisordersmissirenaPas encore d'évaluation
- DMS. K12. DermatopathologyDocument64 pagesDMS. K12. DermatopathologymissirenaPas encore d'évaluation
- DMS. K09b. LeprosyDocument41 pagesDMS. K09b. LeprosymissirenaPas encore d'évaluation
- DMS. K02a. Struktur Dasar Dan Fungsi KulitDocument54 pagesDMS. K02a. Struktur Dasar Dan Fungsi KulitmissirenaPas encore d'évaluation
- DMS. K05. Other Parasitic InfectionsDocument17 pagesDMS. K05. Other Parasitic InfectionsmissirenaPas encore d'évaluation
- Defense MechanismDocument19 pagesDefense MechanismmissirenaPas encore d'évaluation
- Delirium, Dementia, Amnestic & Other Cognitive and Mental KBKDocument18 pagesDelirium, Dementia, Amnestic & Other Cognitive and Mental KBKIndah Permata SariPas encore d'évaluation
- K - 11 Physiology of Pregnancy (Fisiologi)Document46 pagesK - 11 Physiology of Pregnancy (Fisiologi)missirenaPas encore d'évaluation
- K - 13 Perkembangan Morfologi Dan Fungsional Janin (Obgyn)Document53 pagesK - 13 Perkembangan Morfologi Dan Fungsional Janin (Obgyn)missirenaPas encore d'évaluation
- K - 9 Male Reproductive Hormone (Biokimia)Document14 pagesK - 9 Male Reproductive Hormone (Biokimia)missirenaPas encore d'évaluation
- K - 7 & K - 8 Female Reproduction Hormone (Biokimia)Document36 pagesK - 7 & K - 8 Female Reproduction Hormone (Biokimia)missirenaPas encore d'évaluation
- K - 4 Aterioskleoris & Penyakit Jantung Koroner (Fisiologi)Document34 pagesK - 4 Aterioskleoris & Penyakit Jantung Koroner (Fisiologi)missirenaPas encore d'évaluation
- K - 5 Coronary Artery Disease (Kardiologi)Document32 pagesK - 5 Coronary Artery Disease (Kardiologi)missirenaPas encore d'évaluation
- K - 16 Congestive Heart Failure (Fisiologi)Document23 pagesK - 16 Congestive Heart Failure (Fisiologi)missirenaPas encore d'évaluation
- K - 15 Myocarditis (Kardiologi)Document51 pagesK - 15 Myocarditis (Kardiologi)missirenaPas encore d'évaluation
- K - 7 Demam Rematik (Kardiologi)Document40 pagesK - 7 Demam Rematik (Kardiologi)missirenaPas encore d'évaluation
- K - 16 Congestive Heart Failure (Fisiologi)Document23 pagesK - 16 Congestive Heart Failure (Fisiologi)missirenaPas encore d'évaluation
- K - 12 Heart As A Pump (Fisiologi)Document36 pagesK - 12 Heart As A Pump (Fisiologi)missirenaPas encore d'évaluation
- Histology of Cardiovascular System (Histologi)Document57 pagesHistology of Cardiovascular System (Histologi)missirena100% (1)
- Kuliah CardiovascularDocument60 pagesKuliah CardiovascularmissirenaPas encore d'évaluation
- K - 6 Acute Rheumatic FeverDocument31 pagesK - 6 Acute Rheumatic FeverEster SibaraniPas encore d'évaluation
- K - 4 Valvular Heart Disease (Fisiologi)Document19 pagesK - 4 Valvular Heart Disease (Fisiologi)missirenaPas encore d'évaluation
- ACTIVIDAD ANTIOXIDANTE, HIPOLIPEMIANTE y ANTIPLAQUETARIA DEL TOMATE (Solanum Lycopersicum L.) y EL EFECTO DE SU PROCESAMIENTO y ALMACENAJEDocument10 pagesACTIVIDAD ANTIOXIDANTE, HIPOLIPEMIANTE y ANTIPLAQUETARIA DEL TOMATE (Solanum Lycopersicum L.) y EL EFECTO DE SU PROCESAMIENTO y ALMACENAJEsergi batuecas cervantesPas encore d'évaluation
- Clinical Biochemistry - Fifth YearDocument176 pagesClinical Biochemistry - Fifth YearBayan AlsaadiPas encore d'évaluation
- Okuyama Et Al. 2015 - Statins Stimulate Atherosclerosis and Heart Failure, Pharmacological MechanismsDocument11 pagesOkuyama Et Al. 2015 - Statins Stimulate Atherosclerosis and Heart Failure, Pharmacological MechanismsAlbert CalvetPas encore d'évaluation
- The Myths of Vegetarianism: Stephen Byrnes, PHDDocument31 pagesThe Myths of Vegetarianism: Stephen Byrnes, PHDNikita ZhukPas encore d'évaluation
- Nihms 1873457Document15 pagesNihms 1873457Hanssel Viramontes CastroPas encore d'évaluation
- Case Analysis 1Document11 pagesCase Analysis 1Eloisa DanoPas encore d'évaluation
- DietandCVDriskfactorsinBotswana Kwape PhDthesis2012 (1) (001-025)Document25 pagesDietandCVDriskfactorsinBotswana Kwape PhDthesis2012 (1) (001-025)Indri Reskiawanti GalibPas encore d'évaluation
- Respiratory and Circulatory Systems RelationDocument23 pagesRespiratory and Circulatory Systems RelationclarissePas encore d'évaluation
- 2022-Association of iSGLT2 Use With Cardiovascular and Renal Outcomes in Type 2 Diabetes Mellitus Patients With Stabilized AMIDocument8 pages2022-Association of iSGLT2 Use With Cardiovascular and Renal Outcomes in Type 2 Diabetes Mellitus Patients With Stabilized AMIWENDY JOHANA HENRIQUEZ SEGURA ESTUDIANTE ACTIVOPas encore d'évaluation
- The Relationship Between Hypertension and Myocardial Infarction at Haji General Hospital Medan in 2019Document6 pagesThe Relationship Between Hypertension and Myocardial Infarction at Haji General Hospital Medan in 2019International Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- 1 s2.0 S0021915018315259 Main PDFDocument8 pages1 s2.0 S0021915018315259 Main PDFElson TavaresPas encore d'évaluation
- Flash Pulmonary Oedema and Bilateral Renal Artery Stenosis: The Pickering SyndromeDocument8 pagesFlash Pulmonary Oedema and Bilateral Renal Artery Stenosis: The Pickering SyndromeMahmoud DiaaPas encore d'évaluation
- Andreas Kousios, Panayiotis Kouis, Alexandros Hadjivasilis, and Andrie PanayiotouDocument15 pagesAndreas Kousios, Panayiotis Kouis, Alexandros Hadjivasilis, and Andrie Panayiotou7 MNTPas encore d'évaluation
- Acute Coronary Syndrome and Coronary Heart Disease GuideDocument29 pagesAcute Coronary Syndrome and Coronary Heart Disease GuideDwi Akbarina YahyaPas encore d'évaluation
- Abstrac 2222Document19 pagesAbstrac 2222josephmainam9Pas encore d'évaluation
- Describe Effects of Tar and Carcinogens in Smoke On The Respiratory SystemDocument4 pagesDescribe Effects of Tar and Carcinogens in Smoke On The Respiratory SystemNathuAndrewsPas encore d'évaluation