Vous aimerez peut-être aussi
- Dr. Methaq A.M.Hussein: MRCP (London) ,,sce of Endocrine (London) FIBIMS, Professor of Medicine LECT. 1,2Document8 pagesDr. Methaq A.M.Hussein: MRCP (London) ,,sce of Endocrine (London) FIBIMS, Professor of Medicine LECT. 1,2hussain AltaherPas encore d'évaluation
- Anterior Pituitary Gland: Fawwaz Ammari Laith & HaniDocument22 pagesAnterior Pituitary Gland: Fawwaz Ammari Laith & HaniRashed ShatnawiPas encore d'évaluation
- Zoology Notes: 018 Chapter 14Document3 pagesZoology Notes: 018 Chapter 14humanupgrade100% (1)
- PITUITARYDocument37 pagesPITUITARYaparna shamaPas encore d'évaluation
- Endocrine System DiseasesDocument87 pagesEndocrine System DiseasesFahmiArifMuhammadPas encore d'évaluation
- MODULE 2 Disorders of The Pituitary GlandDocument24 pagesMODULE 2 Disorders of The Pituitary GlandLorraine GambitoPas encore d'évaluation
- HypopituitarismDocument2 pagesHypopituitarismAnne de VeraPas encore d'évaluation
- Seminar ON Pituitary DisorderDocument62 pagesSeminar ON Pituitary DisorderZorini ChhangtePas encore d'évaluation
- Part 2 - MEDTERM-117 LECDocument9 pagesPart 2 - MEDTERM-117 LECfrechel kimPas encore d'évaluation
- Hypothalamus - AppliedDocument48 pagesHypothalamus - Appliedameer abdullahPas encore d'évaluation
- Endocrine Pathology - UntadDocument158 pagesEndocrine Pathology - UntadfahrulrozyPas encore d'évaluation
- Endocrine Glands: Hormones Affect Other Endocrine Glands or Body SystemsDocument12 pagesEndocrine Glands: Hormones Affect Other Endocrine Glands or Body SystemsNadzierah RazakPas encore d'évaluation
- Hypopituitarism Group F BSN 3Document21 pagesHypopituitarism Group F BSN 3Mari IllustriousPas encore d'évaluation
- Activity70 HypopituitarismDocument8 pagesActivity70 HypopituitarismJohanna Recca MarinoPas encore d'évaluation
- Hyperpituitarism Group e Bsn3Document17 pagesHyperpituitarism Group e Bsn3Mari IllustriousPas encore d'évaluation
- Article 12Document10 pagesArticle 12WPRN RanasinghePas encore d'évaluation
- Endocrine Gland: Aldrin Mercado Bsae Ii-ADocument3 pagesEndocrine Gland: Aldrin Mercado Bsae Ii-AaldrinPas encore d'évaluation
- Hypothalamus - Anterior Pituitary and Their HormonesDocument138 pagesHypothalamus - Anterior Pituitary and Their HormonesML Rodriguez100% (1)
- UNIT II Endocrine & Metabolic DisordersDocument19 pagesUNIT II Endocrine & Metabolic DisordersAmmar BhattiPas encore d'évaluation
- 11 Biology Revision Study Material Chapter 22 PDFDocument8 pages11 Biology Revision Study Material Chapter 22 PDFSaurav SoniPas encore d'évaluation
- Pathology of The Endocrine System: Causes A. Pituitary Usually Anterior LobeDocument19 pagesPathology of The Endocrine System: Causes A. Pituitary Usually Anterior LobecystanarisaPas encore d'évaluation
- Patologi Endokrin 2016Document132 pagesPatologi Endokrin 2016agusPas encore d'évaluation
- DR Nyoman. Sistem EndokrinDocument93 pagesDR Nyoman. Sistem EndokrinAnnisaPas encore d'évaluation
- Pathophysiology of The Endocrine System. Violation of Hypophysis, Thyroid and Adrenal Glands. General Adaptation SyndromeDocument123 pagesPathophysiology of The Endocrine System. Violation of Hypophysis, Thyroid and Adrenal Glands. General Adaptation SyndromeAyman RehmanPas encore d'évaluation
- Endocrine System Pathology 2009Document195 pagesEndocrine System Pathology 2009SofiaemangintePas encore d'évaluation
- HipopituitarismeDocument5 pagesHipopituitarismeMiftia Yunanda PutriPas encore d'évaluation
- Endocrinology: Elizabeth H., MD. PathologistDocument72 pagesEndocrinology: Elizabeth H., MD. PathologistABUBEKER BESHIRPas encore d'évaluation
- Endocrine System: Practical PartDocument58 pagesEndocrine System: Practical PartAmy AmyPas encore d'évaluation
- Posteria Pituitary 2023 PDFDocument51 pagesPosteria Pituitary 2023 PDFMpho MosehlaPas encore d'évaluation
- Presentation 6Document26 pagesPresentation 6555556666667777777Pas encore d'évaluation
- Inbound 5293281166643491950Document15 pagesInbound 5293281166643491950MUHAMMAD ISHAQPas encore d'évaluation
- Pituitary Hormones and Their Control by The HypothalamusDocument26 pagesPituitary Hormones and Their Control by The HypothalamusDr. AliPas encore d'évaluation
- Anatomy AND Physiology: Endocrine SystemDocument13 pagesAnatomy AND Physiology: Endocrine Systemsaroj karkiPas encore d'évaluation
- Diseases of The Endocrine SystemDocument4 pagesDiseases of The Endocrine SystemJerahmeel Sombilon Genilla100% (1)
- Endocrine System ProvidedDocument73 pagesEndocrine System Providedummezainhumayra11Pas encore d'évaluation
- Pituitary DisorderDocument48 pagesPituitary DisorderAyumi AgungPas encore d'évaluation
- Endocrine SystemDocument43 pagesEndocrine Systemwieka mawiePas encore d'évaluation
- Pituitary GlandDocument9 pagesPituitary GlandS GrayPas encore d'évaluation
- ArooosaDocument20 pagesArooosaMudassir FarooqPas encore d'évaluation
- Endocrine Disorders and The Neurologic ManifestationsDocument49 pagesEndocrine Disorders and The Neurologic ManifestationsAnonymous JWxpPiJf50% (2)
- Sistem Endokrin: Patologi Anatomi FK Unimal Bandar LampungDocument41 pagesSistem Endokrin: Patologi Anatomi FK Unimal Bandar LampungvaliamnisaPas encore d'évaluation
- Endocrine PathologyDocument96 pagesEndocrine PathologyElodie NguetiePas encore d'évaluation
- Hypothyroidism: Prepared By: Angel Shwaihat Enas Khamaiseh Supervised By: Dr. Khalil Al SoutariDocument33 pagesHypothyroidism: Prepared By: Angel Shwaihat Enas Khamaiseh Supervised By: Dr. Khalil Al Soutariraed faisalPas encore d'évaluation
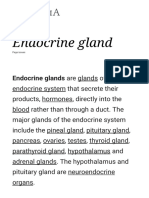
- Endocrine Gland - Wikipedia, The Free EncyclopediaDocument5 pagesEndocrine Gland - Wikipedia, The Free EncyclopediakbhattacPas encore d'évaluation
- Endocrine Gland - WikipediaDocument29 pagesEndocrine Gland - WikipediaSumaya FarheenPas encore d'évaluation
- 40.43.function of Endocrine - Pptx?targetDocument28 pages40.43.function of Endocrine - Pptx?targetAnnemerline RavixPas encore d'évaluation
- Disorders of Endocrine SystemDocument48 pagesDisorders of Endocrine SystemSHARIM ASGHARPas encore d'évaluation
- Uworld EndocrineDocument211 pagesUworld Endocrineهنادي رازمPas encore d'évaluation
- HypothyridismDocument18 pagesHypothyridismanuu1404Pas encore d'évaluation
- Examinations of Endocrine DisordersDocument72 pagesExaminations of Endocrine Disorderskyle otedaPas encore d'évaluation
- EndocrineDocument12 pagesEndocrineAna FelPas encore d'évaluation
- Causes: Sheehan Syndrome, Also Known As Postpartum Hypopituitarism or Postpartum Pituitary NecrosisDocument5 pagesCauses: Sheehan Syndrome, Also Known As Postpartum Hypopituitarism or Postpartum Pituitary NecrosisHyacinth ExmundoPas encore d'évaluation
- III-Skill/Concept Building Exercises: A1 - Directions: Identify The Term Being Described Below. Write Your Answer On The Space ProvidedDocument11 pagesIII-Skill/Concept Building Exercises: A1 - Directions: Identify The Term Being Described Below. Write Your Answer On The Space ProvidedMARIA CHARMIN M. MEJIAPas encore d'évaluation
- Bahir Dar UniversityDocument23 pagesBahir Dar UniversityĎĵ Žě ĤőpėPas encore d'évaluation
- Group 4 - Alteration of Hormonal RegulationDocument17 pagesGroup 4 - Alteration of Hormonal RegulationMarcus KaglPas encore d'évaluation
- Hormones of PituitaryDocument35 pagesHormones of Pituitarybhagirath kansara100% (1)
- Endocrine MorphoDocument102 pagesEndocrine MorphocpPas encore d'évaluation
- Endocrine Disorders 09Document192 pagesEndocrine Disorders 09Dennis ChristopherPas encore d'évaluation
- Hypopituitarism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandHypopituitarism, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Alert Medical Series: Internal Medicine Alert I, II, IIID'EverandAlert Medical Series: Internal Medicine Alert I, II, IIIPas encore d'évaluation
- Bab I LiteratureDocument13 pagesBab I LiteratureNurulDiniaPutriPas encore d'évaluation
- Ejhs2002 0107Document6 pagesEjhs2002 0107zuhrahgiatamahPas encore d'évaluation
- ExelDocument2 pagesExelzuhrahgiatamahPas encore d'évaluation
- Ejhs2002 0107Document6 pagesEjhs2002 0107zuhrahgiatamahPas encore d'évaluation
- X Ipa 2 GanjilDocument2 pagesX Ipa 2 GanjilzuhrahgiatamahPas encore d'évaluation
- Pengertian Literature ReviewDocument4 pagesPengertian Literature ReviewzuhrahgiatamahPas encore d'évaluation
- Cancel Fuel Rise (Esp)Document4 pagesCancel Fuel Rise (Esp)zuhrahgiatamahPas encore d'évaluation
- EspDocument2 pagesEspzuhrahgiatamahPas encore d'évaluation
- Daily ActivityDocument2 pagesDaily ActivityzuhrahgiatamahPas encore d'évaluation
- Group 1 DebateDocument3 pagesGroup 1 DebatezuhrahgiatamahPas encore d'évaluation
- 2013 Article 3273Document6 pages2013 Article 3273zuhrahgiatamahPas encore d'évaluation
- Once Upon TimeDocument6 pagesOnce Upon TimezuhrahgiatamahPas encore d'évaluation
- Aetiology,: THE Prevention Treatment of SimpleDocument6 pagesAetiology,: THE Prevention Treatment of SimplezuhrahgiatamahPas encore d'évaluation
- In The Name of LoveDocument4 pagesIn The Name of LovezuhrahgiatamahPas encore d'évaluation
- Bac GroundDocument2 pagesBac GroundzuhrahgiatamahPas encore d'évaluation
- Ni Hms 58309Document5 pagesNi Hms 58309zuhrahgiatamahPas encore d'évaluation
- Interview Oleh ZuhrahDocument1 pageInterview Oleh ZuhrahzuhrahgiatamahPas encore d'évaluation
- JPM 04 00200Document21 pagesJPM 04 00200zuhrahgiatamahPas encore d'évaluation
- Bac GroundDocument2 pagesBac GroundzuhrahgiatamahPas encore d'évaluation
- Bac GroundDocument2 pagesBac GroundzuhrahgiatamahPas encore d'évaluation
- Antepartum 2Document3 pagesAntepartum 2Emily Davis100% (2)
- Anatomy and Physiology of The Reproductive SystemDocument31 pagesAnatomy and Physiology of The Reproductive SystemYUAN CAÑAS100% (1)
- HL BIOLOGY PAST QUESTIONS PAPER PrintingDocument192 pagesHL BIOLOGY PAST QUESTIONS PAPER PrintingFaizaPas encore d'évaluation
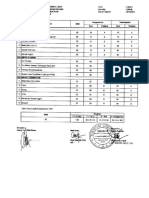
- Department of Biochemistry: Test Name Value Unit Bio. Ref IntervalDocument18 pagesDepartment of Biochemistry: Test Name Value Unit Bio. Ref IntervalTabitha MartynPas encore d'évaluation
- Human Brain DevelopmentDocument9 pagesHuman Brain DevelopmentAnna ChalupkaPas encore d'évaluation
- Clearblue Pregnancy Test With Conception Indicator BrochureDocument12 pagesClearblue Pregnancy Test With Conception Indicator Brochuremanda84Pas encore d'évaluation
- 2012 O&Gsoc BGDA Revision TutorialDocument53 pages2012 O&Gsoc BGDA Revision TutorialAndrew CheongPas encore d'évaluation
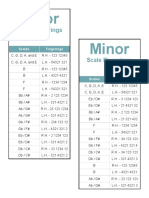
- Scales and Arpeggios FingeringsDocument2 pagesScales and Arpeggios FingeringsJames RileyPas encore d'évaluation
- Teza de Doctorat - DR - Goel-SemnatDocument150 pagesTeza de Doctorat - DR - Goel-Semnatpopescu ancaPas encore d'évaluation
- Module 3Document20 pagesModule 3VENTURA, ANNIE M.Pas encore d'évaluation
- Placenta Previa Case StudyDocument59 pagesPlacenta Previa Case StudySiergs Smith GervacioPas encore d'évaluation
- 0 Pharmacology - Presentation.by - SIDRADocument29 pages0 Pharmacology - Presentation.by - SIDRASidra AlamPas encore d'évaluation
- Part 1Document27 pagesPart 1Kian AliPas encore d'évaluation
- Respon Pemberian Ekstrak Hipofisa Ayam Broiler Terhadap Waktu LatensiDocument7 pagesRespon Pemberian Ekstrak Hipofisa Ayam Broiler Terhadap Waktu LatensiendayaniPas encore d'évaluation
- Midterm Exams - AnatomyDocument9 pagesMidterm Exams - AnatomyBing58Pas encore d'évaluation
- PATH All TA Reviews Answers and Notes11Document718 pagesPATH All TA Reviews Answers and Notes11Andleeb Imran100% (1)
- Artificial Insemination ManualDocument54 pagesArtificial Insemination ManualSteve Cris SanchezPas encore d'évaluation
- STPM BIOLOGY Hormone/Chemical CoordinationDocument21 pagesSTPM BIOLOGY Hormone/Chemical Coordinationwkwhui100% (4)
- B11.5 Hormones in The Menstrual Cycle AnswersDocument4 pagesB11.5 Hormones in The Menstrual Cycle AnswersBenjamin WatsonPas encore d'évaluation
- Biology Paper 1, 2, 3 Trial SPM 2011 MRSMDocument86 pagesBiology Paper 1, 2, 3 Trial SPM 2011 MRSMSashaSparksPas encore d'évaluation
- Hormone 4Document1 pageHormone 4Kehmily SucgangPas encore d'évaluation
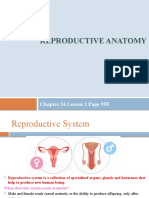
- Reproductive Anatomy: Chapter 34 Lesson 1 Page 958Document13 pagesReproductive Anatomy: Chapter 34 Lesson 1 Page 958JanaPas encore d'évaluation
- Revision Test-07: For NEET-2022 Answer KeyDocument11 pagesRevision Test-07: For NEET-2022 Answer KeykrishnaPas encore d'évaluation
- Reproductive Health Sexual HealthDocument8 pagesReproductive Health Sexual HealthVenus Anne LamayoPas encore d'évaluation
- Science 10 Quarter 2 Key of CorrectionDocument7 pagesScience 10 Quarter 2 Key of CorrectionDaisy Soriano PrestozaPas encore d'évaluation
- Activity 4 - Male Reproductive SystemDocument17 pagesActivity 4 - Male Reproductive Systemisabellamarie.castillo.crsPas encore d'évaluation
- Biologi Gonzaga - Hormon WanitaDocument9 pagesBiologi Gonzaga - Hormon WanitaVinna ZulhelmiPas encore d'évaluation
- Estevia en Tratamiento de Diabates en Ratas PDFDocument8 pagesEstevia en Tratamiento de Diabates en Ratas PDFjuan de Dios Limachi OchoaPas encore d'évaluation
- Menstrual Cycle Test 1 1Document8 pagesMenstrual Cycle Test 1 1KvmLly100% (1)
- 2013 Maternal and Child Health Nursing Reviewer CompleteDocument40 pages2013 Maternal and Child Health Nursing Reviewer CompleteHarley Justiniani Dela CruzPas encore d'évaluation