Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Goals Editable PDFDocument140 pagesGoals Editable PDFManuel Ascanio67% (3)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- QRF HD785-7Document2 pagesQRF HD785-7Ralf MaurerPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Wood Lamp Skin ExaminationDocument4 pagesWood Lamp Skin ExaminationNungky Rizkia Dewi100% (1)
- GCSDocument20 pagesGCSnicole aligno100% (2)
- Ignition System Spark Test DiagnosisDocument24 pagesIgnition System Spark Test DiagnosisMohamed l'Amine75% (4)
- Cement ReportDocument86 pagesCement ReportSohaibPas encore d'évaluation
- Parasitology Lecture Hosts, Symbiosis & TransmissionDocument10 pagesParasitology Lecture Hosts, Symbiosis & TransmissionPatricia Ann JosePas encore d'évaluation
- PT6 Training ManualDocument64 pagesPT6 Training ManualAnderson Guimarães100% (2)
- Scaffolding Control & MeasuresDocument3 pagesScaffolding Control & Measuresviswamanoj100% (1)
- Activity No 1 - Hydrocyanic AcidDocument4 pagesActivity No 1 - Hydrocyanic Acidpharmaebooks100% (2)
- EndokrinDocument4 pagesEndokrinNungky Rizkia DewiPas encore d'évaluation
- EndokrinDocument4 pagesEndokrinNungky Rizkia DewiPas encore d'évaluation
- Heart EksDocument11 pagesHeart EksAndri FerdianPas encore d'évaluation
- Abses HeparDocument1 pageAbses HeparNungky Rizkia DewiPas encore d'évaluation
- Seizure Frequency During PregnancyDocument9 pagesSeizure Frequency During PregnancyNungky Rizkia DewiPas encore d'évaluation
- Kontra Obat TBDocument4 pagesKontra Obat TBNungky Rizkia DewiPas encore d'évaluation
- AntibioticDocument4 pagesAntibioticionanic72Pas encore d'évaluation
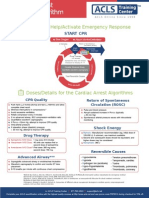
- Shout For Help/Activate Emergency Response: CPR StartDocument2 pagesShout For Help/Activate Emergency Response: CPR StartdavpierPas encore d'évaluation
- GINA Pocket2013 May15Document0 pageGINA Pocket2013 May15David BarzalloPas encore d'évaluation
- Excretory System PresentationDocument32 pagesExcretory System PresentationNungky Rizkia DewiPas encore d'évaluation
- A&P 2 - Digestive System Flashcards - QuizletDocument1 pageA&P 2 - Digestive System Flashcards - QuizletMunachande KanondoPas encore d'évaluation
- Válvulas Flomatic USADocument40 pagesVálvulas Flomatic USAEfrain DuartePas encore d'évaluation
- Indonesia Organic Farming 2011 - IndonesiaDOCDocument18 pagesIndonesia Organic Farming 2011 - IndonesiaDOCJamal BakarPas encore d'évaluation
- Nursing Plan of Care Concept Map - Immobility - Hip FractureDocument2 pagesNursing Plan of Care Concept Map - Immobility - Hip Fracturedarhuynh67% (6)
- Pet - WikipediaDocument12 pagesPet - Wikipediabdalcin5512Pas encore d'évaluation
- Slaked Lime MSDS Safety SummaryDocument7 pagesSlaked Lime MSDS Safety SummaryFurqan SiddiquiPas encore d'évaluation
- Frank Wood S Business Accounting 1Document13 pagesFrank Wood S Business Accounting 1Kofi AsaasePas encore d'évaluation
- Live Performance Award Ma000081 Pay GuideDocument48 pagesLive Performance Award Ma000081 Pay GuideDan LijndersPas encore d'évaluation
- Guide Propedevt Stomat 2c EngDocument256 pagesGuide Propedevt Stomat 2c EngJhoel Jhonatan Torres MuñozPas encore d'évaluation
- 2024 - Chung 2024 Flexible Working and Gender Equality R2 CleanDocument123 pages2024 - Chung 2024 Flexible Working and Gender Equality R2 CleanmariaPas encore d'évaluation
- OC - PlumberDocument6 pagesOC - Plumbertakuva03Pas encore d'évaluation
- 57882d4608ae21394a0c7b00 PDFDocument574 pages57882d4608ae21394a0c7b00 PDFtualaPas encore d'évaluation
- Alok ResumeDocument3 pagesAlok Resumealok choudharyPas encore d'évaluation
- Apc 8x Install Config Guide - rn0 - LT - enDocument162 pagesApc 8x Install Config Guide - rn0 - LT - enOney Enrique Mendez MercadoPas encore d'évaluation
- Case Report on Right Knee FuruncleDocument47 pagesCase Report on Right Knee Furuncle馮宥忻Pas encore d'évaluation
- Introduction To Animal Science For Plant ScienceDocument63 pagesIntroduction To Animal Science For Plant ScienceJack OlanoPas encore d'évaluation
- Funds Flow Statement ExplainedDocument76 pagesFunds Flow Statement Explainedthella deva prasad0% (1)
- TA-Ingles IX - UAPDocument10 pagesTA-Ingles IX - UAPmanuel brennerPas encore d'évaluation
- Diagnostic and Statistical Manual of Mental Disorders: Distinction From ICD Pre-DSM-1 (1840-1949)Document25 pagesDiagnostic and Statistical Manual of Mental Disorders: Distinction From ICD Pre-DSM-1 (1840-1949)Unggul YudhaPas encore d'évaluation
- Lease Practice QuestionsDocument4 pagesLease Practice QuestionsAbdul SamiPas encore d'évaluation
- Manual Masina de Spalat Slim SamsungDocument1 020 pagesManual Masina de Spalat Slim SamsungPerfectreviewPas encore d'évaluation