Vous aimerez peut-être aussi
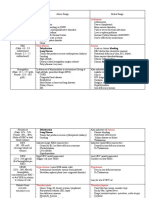
- Warm and Cold Type of IHADocument2 pagesWarm and Cold Type of IHAHanisha EricaPas encore d'évaluation
- ParasitologyDocument5 pagesParasitologyHanisha EricaPas encore d'évaluation
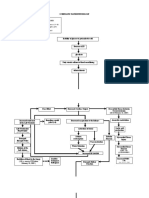
- Schematic Pathophysiology Predisposing FactorsDocument7 pagesSchematic Pathophysiology Predisposing FactorsHanisha EricaPas encore d'évaluation
- Schematic Pa Tho Physiology Ms1Document4 pagesSchematic Pa Tho Physiology Ms1Hanisha EricaPas encore d'évaluation
- Hand Hygiene and The Prevalence and Intensity of AscariasisDocument19 pagesHand Hygiene and The Prevalence and Intensity of AscariasisHanisha EricaPas encore d'évaluation
- March 30Document4 pagesMarch 30Hanisha EricaPas encore d'évaluation
- Physical Assessment: Vital SignsDocument8 pagesPhysical Assessment: Vital SignsHanisha EricaPas encore d'évaluation
- Use of and Attitudes and Knowledge About Pap Smears Among Women in KuwaitDocument18 pagesUse of and Attitudes and Knowledge About Pap Smears Among Women in KuwaitHanisha EricaPas encore d'évaluation
- Knowledge of Selected Nurses and Clinical InstructorsDocument13 pagesKnowledge of Selected Nurses and Clinical InstructorsHanisha EricaPas encore d'évaluation
- Para ReportDocument21 pagesPara ReportHanisha EricaPas encore d'évaluation
- Phylum Sarcomas Ti Gop HoraDocument38 pagesPhylum Sarcomas Ti Gop HoraHanisha EricaPas encore d'évaluation
- DX Test ms1Document4 pagesDX Test ms1Hanisha EricaPas encore d'évaluation
- Entamoeba ColiDocument14 pagesEntamoeba ColiHanisha Erica100% (1)
- Heterophyid FlukesDocument2 pagesHeterophyid FlukesHanisha EricaPas encore d'évaluation
- Paragonimus WestermaniDocument3 pagesParagonimus WestermaniHanisha EricaPas encore d'évaluation
- Fasciolopsis BuskiDocument2 pagesFasciolopsis BuskiHanisha Erica100% (1)
- Echinostoma IlocanumDocument2 pagesEchinostoma IlocanumHanisha EricaPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Market Analysis of Biosensors For Food Safety: Industry ReviewDocument6 pagesMarket Analysis of Biosensors For Food Safety: Industry ReviewHai HuyPas encore d'évaluation
- Partial Genome Characterization of Novel ParapoxviDocument4 pagesPartial Genome Characterization of Novel Parapoxviali zohaibPas encore d'évaluation
- Anti HBC Total II 30314Document6 pagesAnti HBC Total II 30314armada thamPas encore d'évaluation
- Pediatric Community Acquired Pneumonia Case StudyDocument17 pagesPediatric Community Acquired Pneumonia Case StudyMary Ann Credo Manlangit100% (2)
- Sample Question Paper PDFDocument20 pagesSample Question Paper PDFMahesh SharmaPas encore d'évaluation
- Root Cause AnalysisDocument1 pageRoot Cause AnalysisTri Hastuti HendrayaniPas encore d'évaluation
- IMY Unit 1, Sub Unit 1.1Document11 pagesIMY Unit 1, Sub Unit 1.1fdvfsgffefPas encore d'évaluation
- Anthelmintic DrugsDocument35 pagesAnthelmintic DrugsRamla KashifPas encore d'évaluation
- 3 Session 3 - AbdominalExamDocument15 pages3 Session 3 - AbdominalExamjhk0428Pas encore d'évaluation
- 10 List of Bacterial Infections MHEA NICOLE SALCEDO NEWDocument56 pages10 List of Bacterial Infections MHEA NICOLE SALCEDO NEWMhea Nicole SalcedoPas encore d'évaluation
- Skyline Plots PDFDocument35 pagesSkyline Plots PDFMarijaTodorovicPas encore d'évaluation
- Oral Cavity Is The Mirror of Your Own BodyDocument60 pagesOral Cavity Is The Mirror of Your Own BodyNazia AliPas encore d'évaluation
- AP2 Unit 6 Exam Review CASDocument12 pagesAP2 Unit 6 Exam Review CASMarera DomnicPas encore d'évaluation
- IRS Group OET Reading Part ADocument5 pagesIRS Group OET Reading Part ADaham MothanaPas encore d'évaluation
- Vaksin Covid WhoDocument30 pagesVaksin Covid WhoMami PapiPas encore d'évaluation
- The Vaccination Fraud: Transcript Reveals DangersDocument17 pagesThe Vaccination Fraud: Transcript Reveals DangersC.K.Pas encore d'évaluation
- BAKUNADocument16 pagesBAKUNAJamesPas encore d'évaluation
- Haemolytica, Alcaligenes Faecalis) - in General, Bacte-: ActeriaDocument35 pagesHaemolytica, Alcaligenes Faecalis) - in General, Bacte-: ActeriaMonik TanPas encore d'évaluation
- Restriction EnzymeDocument45 pagesRestriction Enzymedrsubhash81Pas encore d'évaluation
- Case Report: Management of Dairy Farm: Klebsiella SPP Mastitis On ADocument9 pagesCase Report: Management of Dairy Farm: Klebsiella SPP Mastitis On ApramiswariPas encore d'évaluation
- Epstein-Barr Virus (Infectious Mononucleosis)Document3 pagesEpstein-Barr Virus (Infectious Mononucleosis)KanayaPas encore d'évaluation
- Drug StudyDocument6 pagesDrug StudyDsquared100% (1)
- Sbi3u Mini Test 2 Unit 1 AnswersDocument2 pagesSbi3u Mini Test 2 Unit 1 Answerschriston.mPas encore d'évaluation
- Roosendaal Study of Vaccinated vs. Unvaccinated Children in The Netherlands: Results SurveyDocument4 pagesRoosendaal Study of Vaccinated vs. Unvaccinated Children in The Netherlands: Results Surveythomas_austin_189% (9)
- Management of HIV/AIDS by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaDocument13 pagesManagement of HIV/AIDS by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaSreekrishnan TrikkurPas encore d'évaluation
- CBC reference ranges and abnormal conditionsDocument4 pagesCBC reference ranges and abnormal conditionsndrfernandezPas encore d'évaluation
- Bacteriological Profile of Infections in Burns Unit - Plastic and Reconstructive Surgery Department - Mohammed Vi Chu MarrakechDocument7 pagesBacteriological Profile of Infections in Burns Unit - Plastic and Reconstructive Surgery Department - Mohammed Vi Chu MarrakechIJAR JOURNALPas encore d'évaluation
- Wood Lamp Examination: A Forgotten Diagnostic ToolDocument1 pageWood Lamp Examination: A Forgotten Diagnostic ToolBenvenuto AxelPas encore d'évaluation
- A4 Size MC3 Midterms ReviewerDocument9 pagesA4 Size MC3 Midterms ReviewerEl Grace EligedoPas encore d'évaluation
- Philippine high school exam on Southeast Asian culture and musicDocument3 pagesPhilippine high school exam on Southeast Asian culture and musicjanice m. gasparPas encore d'évaluation