Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Test Bank For Introduction To Critical Care Nursing 7th Edition by SoleDocument6 pagesTest Bank For Introduction To Critical Care Nursing 7th Edition by SoleDonnie Torris100% (34)
- West Florida Regional Medical Centre111Document73 pagesWest Florida Regional Medical Centre111Shashi Yadav100% (1)
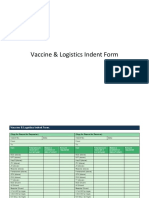
- Indent FormDocument2 pagesIndent FormDheeraj Bhatt0% (1)
- History Back PainDocument3 pagesHistory Back PaindrwiraPas encore d'évaluation
- CV Elective Program For International StudentsDocument5 pagesCV Elective Program For International StudentsYosafatPrasetyadiPas encore d'évaluation
- Inflammatory Bowel DiseaseDocument15 pagesInflammatory Bowel DiseaseYanushka Bruce HerathPas encore d'évaluation
- Proforma A1: Residential/Domicile CertificateDocument5 pagesProforma A1: Residential/Domicile CertificateRahul RoyPas encore d'évaluation
- ImmerciDocument14 pagesImmercitextilessathishPas encore d'évaluation
- Organon of Homoeopathy by HahnemannDocument246 pagesOrganon of Homoeopathy by HahnemannRajesh Rajendran100% (3)
- Jurnal Promkes 1Document20 pagesJurnal Promkes 1Djamnur AgnessiaPas encore d'évaluation
- Janelle Cabida Supnad BSN 3CDocument2 pagesJanelle Cabida Supnad BSN 3CJanelle Cabida SupnadPas encore d'évaluation
- Responsible Parenthood and Reproductive Health Act of 2012Document22 pagesResponsible Parenthood and Reproductive Health Act of 2012Janette Anne Reyes MacaraigPas encore d'évaluation
- Fall Health & Wellness (October 2022)Document20 pagesFall Health & Wellness (October 2022)Watertown Daily TimesPas encore d'évaluation
- Myusdoctor 150414122940 Conversion Gate01Document15 pagesMyusdoctor 150414122940 Conversion Gate01shipletPas encore d'évaluation
- Draft Jadwal Rapid Pekerja RU V-Dikonversi PDFDocument70 pagesDraft Jadwal Rapid Pekerja RU V-Dikonversi PDFMuhammad sadadPas encore d'évaluation
- Hazard SurveillanceDocument14 pagesHazard SurveillanceAYU LESTARI DARTI AKHSAPas encore d'évaluation
- Patient Complaints in HealthcareDocument12 pagesPatient Complaints in HealthcaresanaaPas encore d'évaluation
- Pneumonia in Children: by DR L N Gachare Paediatrician/PulmonologistDocument35 pagesPneumonia in Children: by DR L N Gachare Paediatrician/PulmonologistAlvin OmondiPas encore d'évaluation
- The Effects of A Postural Supporting "New Nesting Device" On EarlyDocument9 pagesThe Effects of A Postural Supporting "New Nesting Device" On EarlymeritabasrilPas encore d'évaluation
- Drug Study FinalDocument12 pagesDrug Study FinalAna Mae MonteronPas encore d'évaluation
- Dr. Ali Irani: Keynote Address-10:30-11:00 AmDocument2 pagesDr. Ali Irani: Keynote Address-10:30-11:00 Amsiddhartha senPas encore d'évaluation
- Efecto de La Psicoeducación en Muejeres Que Realizan Estudios de MamografiaDocument14 pagesEfecto de La Psicoeducación en Muejeres Que Realizan Estudios de MamografiaJessicaPas encore d'évaluation
- Artificial MethodsDocument23 pagesArtificial MethodsJanna Broqueza RodriguezPas encore d'évaluation
- Tmi - Hiv Aids Workplace Policy and ProgramDocument4 pagesTmi - Hiv Aids Workplace Policy and ProgramGuilliam RoquePas encore d'évaluation
- Publication November 13, 2019Document4 pagesPublication November 13, 2019ZyrinePas encore d'évaluation
- Drug Study, NCP, and Discharge Plan For AppendectomyDocument12 pagesDrug Study, NCP, and Discharge Plan For AppendectomyApril80% (5)
- Evidence Based-How To Ask An Answerable QuestionsDocument62 pagesEvidence Based-How To Ask An Answerable QuestionsFeniPas encore d'évaluation
- RFP For cMYP Development in Pakistan and Other CountriesDocument4 pagesRFP For cMYP Development in Pakistan and Other Countriesisty5nntPas encore d'évaluation
- Erythroderma in Adults - UpToDateDocument39 pagesErythroderma in Adults - UpToDateGusti Ngurah PPas encore d'évaluation
- FWCQ22 COVID19 Healthcare Protocol V28 EnglishDocument24 pagesFWCQ22 COVID19 Healthcare Protocol V28 EnglishKarthik KothandaramanPas encore d'évaluation