Vous aimerez peut-être aussi
- Opioid Pharmacology Definitions: N-CH 3 N-CH 3Document13 pagesOpioid Pharmacology Definitions: N-CH 3 N-CH 3Louis Fortunato100% (1)
- Lecture 16-17 - Opioids AnalgesicsDocument20 pagesLecture 16-17 - Opioids AnalgesicsJedoPas encore d'évaluation
- Drugs of Abuse: OpioidDocument35 pagesDrugs of Abuse: Opioidmalak amerPas encore d'évaluation
- Endogenous Opioid Peptides and Their ReceptorsDocument41 pagesEndogenous Opioid Peptides and Their ReceptorsSayan NagPas encore d'évaluation
- L P 5 Analgesics Final - 22Document32 pagesL P 5 Analgesics Final - 22Zakria Al-HadadPas encore d'évaluation
- Opioid DrugsDocument12 pagesOpioid DrugsSF170riyandaPas encore d'évaluation
- Opioid Analgesics & Antagonists: Dr. Hayder B Sahib Ph.D. PharmacologyDocument47 pagesOpioid Analgesics & Antagonists: Dr. Hayder B Sahib Ph.D. Pharmacologyarham pirachaPas encore d'évaluation
- Medical University of Sofia, Faculty of Medicine Department of Pharmacology and ToxicologyDocument51 pagesMedical University of Sofia, Faculty of Medicine Department of Pharmacology and ToxicologyAMIN THAWABTEHPas encore d'évaluation
- Opoid AnalgesicsDocument29 pagesOpoid AnalgesicsShivsharan100% (1)
- 6 OpioidsDocument23 pages6 Opioidsphoto copyhemnPas encore d'évaluation
- Drugs Acting On Central Nervous SystemDocument59 pagesDrugs Acting On Central Nervous SystemHajrah SuhardiPas encore d'évaluation
- Lect 10 - Opioids and LADocument40 pagesLect 10 - Opioids and LARaneem ShiferPas encore d'évaluation
- Opioid Analgesics and AntagonistsDocument61 pagesOpioid Analgesics and AntagonistsJia YingPas encore d'évaluation
- Opioid AnalgesicDocument43 pagesOpioid AnalgesicAnanta MiaPas encore d'évaluation
- Opioid Receptor Agonists and AntagonistsDocument22 pagesOpioid Receptor Agonists and AntagonistsSiddharth Anand80% (5)
- 2024-02-29 - 1 - Lecture 16-Opioid Analgesics - Lecture NotesDocument14 pages2024-02-29 - 1 - Lecture 16-Opioid Analgesics - Lecture Notesbaf49411Pas encore d'évaluation
- ANALGESIC DRUGS (DR - Dlawer)Document37 pagesANALGESIC DRUGS (DR - Dlawer)OMAR NASSERPas encore d'évaluation
- Opioid AnalgesicDocument12 pagesOpioid AnalgesicFaria Islam JuhiPas encore d'évaluation
- Stupor (Semiconscious) or Insensibility: Endogounus OpioidDocument11 pagesStupor (Semiconscious) or Insensibility: Endogounus OpioidAhmed OsamaPas encore d'évaluation
- Anes DLR Feb 22 2023Document7 pagesAnes DLR Feb 22 2023Benjune RoseladaPas encore d'évaluation
- What are Opioids? Understanding their Uses, Actions and Side EffectsDocument16 pagesWhat are Opioids? Understanding their Uses, Actions and Side EffectsSanthosh Krishna RajanPas encore d'évaluation
- 6.2 Opioid & Non-OpioidsDocument18 pages6.2 Opioid & Non-OpioidsAsem AlhazmiPas encore d'évaluation
- Pain Therapy: by Dr. Hesham GhareebDocument52 pagesPain Therapy: by Dr. Hesham GhareebHesham hfghareebPas encore d'évaluation
- Opiod Analgesics &antagonistsDocument58 pagesOpiod Analgesics &antagonistsVictoria ChepkorirPas encore d'évaluation
- Opioid AnalgesicsDocument27 pagesOpioid AnalgesicsDivya VarsiniPas encore d'évaluation
- OpiodsDocument15 pagesOpiodssash34Pas encore d'évaluation
- Analgesik Opiod - D3anfarDocument66 pagesAnalgesik Opiod - D3anfarnoor cahayaPas encore d'évaluation
- AnalgesicDocument62 pagesAnalgesicAnjum IslamPas encore d'évaluation
- Opioid Analgesics & Antagonists SummaryDocument47 pagesOpioid Analgesics & Antagonists SummaryAli MohamedPas encore d'évaluation
- Opioid Analgesics: Types, Mechanisms and Clinical UsesDocument48 pagesOpioid Analgesics: Types, Mechanisms and Clinical UsesAmiraBenhammou100% (1)
- Narcotic Analgesics - Notes - SY B. PharmaDocument12 pagesNarcotic Analgesics - Notes - SY B. PharmaSneha charakPas encore d'évaluation
- 404T Opioid Analgesics and AntagonistDocument14 pages404T Opioid Analgesics and AntagonistRaja RajaPas encore d'évaluation
- OpiodDocument15 pagesOpiodlandita683Pas encore d'évaluation
- 64 Pharmacology of Opioids Part IDocument7 pages64 Pharmacology of Opioids Part Itamikanji100% (1)
- Lecture 2 Opoid Analgesics PDFDocument12 pagesLecture 2 Opoid Analgesics PDFAbdelrahman WaelPas encore d'évaluation
- Opioids: Dr. Yuri Clement, Pharmacology Unit, FMSDocument40 pagesOpioids: Dr. Yuri Clement, Pharmacology Unit, FMSUnixa BraunPas encore d'évaluation
- CHAPTER 19 Narcotic Analgesics: I General ConsiderationDocument51 pagesCHAPTER 19 Narcotic Analgesics: I General Considerationapi-19916399Pas encore d'évaluation
- Opioid Analgesics & AntagonistsDocument13 pagesOpioid Analgesics & AntagonistsafiniherlyanaPas encore d'évaluation
- Pharmacology - Opioids - The Lecturio Online Medical LibraryDocument10 pagesPharmacology - Opioids - The Lecturio Online Medical Libraryjean PiedraPas encore d'évaluation
- 05 Friedman 2020 Opiods ReviewDocument15 pages05 Friedman 2020 Opiods ReviewJorge GomezPas encore d'évaluation
- Opioids 160224153327Document27 pagesOpioids 160224153327Dr.Aman SaxenaPas encore d'évaluation
- Presented byDocument71 pagesPresented byRun HajPas encore d'évaluation
- Opioid Analgesics & Antagonists: Classification, Mechanisms of Action and Clinical UsesDocument47 pagesOpioid Analgesics & Antagonists: Classification, Mechanisms of Action and Clinical UsesPrincewill SeiyefaPas encore d'évaluation
- AP Dr. Marlar Myint: Narcotic (Opioid) AnalgesicsDocument69 pagesAP Dr. Marlar Myint: Narcotic (Opioid) AnalgesicsHiitachin HikaoruPas encore d'évaluation
- Opioid AnalgesicsDocument53 pagesOpioid AnalgesicsMansi Sanjeev BuddhPas encore d'évaluation
- OpioidsDocument29 pagesOpioidsHassan Jahangir100% (1)
- Pharmacological Control of PainDocument9 pagesPharmacological Control of Painn28h7sr2bmPas encore d'évaluation
- Narcotics Abuse Spring 2021Document51 pagesNarcotics Abuse Spring 2021Fatma HishamPas encore d'évaluation
- Intoksikasi OpioidDocument29 pagesIntoksikasi OpioidAviv Aziz TrionoPas encore d'évaluation
- AnalgesicDocument56 pagesAnalgesicMuhammad hilmiPas encore d'évaluation
- Intrathecal MorphineDocument6 pagesIntrathecal MorphineJoana MoreiraPas encore d'évaluation
- Drugs in ICUDocument83 pagesDrugs in ICUJennifer DixonPas encore d'évaluation
- Pharmacology of Opioids: Maher Khdour, Msc. PHD Clinical PharmacyDocument66 pagesPharmacology of Opioids: Maher Khdour, Msc. PHD Clinical PharmacyYousef JafarPas encore d'évaluation
- Analgesia and AnalgesicsDocument113 pagesAnalgesia and Analgesicsdr_shilpakokate9368Pas encore d'évaluation
- 23 - Pharma. - د. شامل 7Document10 pages23 - Pharma. - د. شامل 7Hassan AdnanPas encore d'évaluation
- General Anesthetics AgentsDocument42 pagesGeneral Anesthetics AgentsHamid Hussain HamidPas encore d'évaluation
- Learning Hypnosis - Hypnosis Application for Coaches and TherapistsD'EverandLearning Hypnosis - Hypnosis Application for Coaches and TherapistsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Exposing the Shameful Face of Drug Addiction: Unveiling the trick behind drug addictionD'EverandExposing the Shameful Face of Drug Addiction: Unveiling the trick behind drug addictionPas encore d'évaluation
- GIFTED: Genetic Information For Treating Eating DisordersD'EverandGIFTED: Genetic Information For Treating Eating DisordersPas encore d'évaluation
- Chapter 8 Cholinocelptor Blocking Drugs-Jjl.2013.9Document44 pagesChapter 8 Cholinocelptor Blocking Drugs-Jjl.2013.9king_goldPas encore d'évaluation
- Diutetics PPT T CHINESEDocument58 pagesDiutetics PPT T CHINESEking_goldPas encore d'évaluation
- Calcium Channel BlockersDocument33 pagesCalcium Channel Blockersking_goldPas encore d'évaluation
- 20 NsaidDocument49 pages20 Nsaidking_goldPas encore d'évaluation
- Arrhythmias and Anti-Arrhythmics: Alex F. Chen, MD, PHD, Faha Professor and Dean School of PharmacyDocument47 pagesArrhythmias and Anti-Arrhythmics: Alex F. Chen, MD, PHD, Faha Professor and Dean School of Pharmacyking_goldPas encore d'évaluation
- Anti ParkinsonDocument29 pagesAnti Parkinsonking_gold100% (1)
- Antiepileptic DrugsDocument39 pagesAntiepileptic Drugsking_goldPas encore d'évaluation
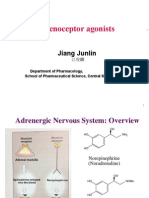
- Adrenoceptor Agonist and Antagonist Drugs-2014.10.7pptDocument83 pagesAdrenoceptor Agonist and Antagonist Drugs-2014.10.7pptking_gold100% (1)
- Bibliography TransplantationDocument56 pagesBibliography Transplantationking_goldPas encore d'évaluation
- Abdominal MassDocument17 pagesAbdominal Mass13un391543Pas encore d'évaluation
- SedativeDocument35 pagesSedativeking_goldPas encore d'évaluation
- 400080Document88 pages400080cndy31Pas encore d'évaluation
- Essentials of Chinese Acupuncture: A Concise GuideDocument448 pagesEssentials of Chinese Acupuncture: A Concise GuideShea-Baby Sheabutterproducts100% (2)
- Drugs Used in The Treatment of Psychoses: Department of Pharmacology, CSU Zhang XiaojieDocument32 pagesDrugs Used in The Treatment of Psychoses: Department of Pharmacology, CSU Zhang Xiaojieking_goldPas encore d'évaluation
- Tahal 4Document15 pagesTahal 4king_goldPas encore d'évaluation
- Sathi 3Document19 pagesSathi 3king_goldPas encore d'évaluation
- Ghalb 3Document20 pagesGhalb 3king_goldPas encore d'évaluation
- Divareh 3Document18 pagesDivareh 3king_goldPas encore d'évaluation
- Omghi 3Document27 pagesOmghi 3king_goldPas encore d'évaluation
- Pankeras 3Document17 pagesPankeras 3king_goldPas encore d'évaluation
- Divar 3Document10 pagesDivar 3king_goldPas encore d'évaluation
- Hofrep 3Document13 pagesHofrep 3king_goldPas encore d'évaluation
- Hofrei 3Document34 pagesHofrei 3king_goldPas encore d'évaluation
- Khalf 2Document13 pagesKhalf 2king_goldPas encore d'évaluation
- Maintenance of Priority Medical Equipment in The Context of Covid-19Document70 pagesMaintenance of Priority Medical Equipment in The Context of Covid-19Noel BuenconsejoPas encore d'évaluation
- 500 Quotes From Heaven - Life-Changing Quotes That Reveal The Wisdom & Power of Near-Death ExperiencesDocument243 pages500 Quotes From Heaven - Life-Changing Quotes That Reveal The Wisdom & Power of Near-Death Experiencesjan75% (4)
- Diseases of The Lid TumorsDocument10 pagesDiseases of The Lid TumorsEliza IancuPas encore d'évaluation
- Web Annex e AnswerkeyDocument21 pagesWeb Annex e AnswerkeyYael EzraPas encore d'évaluation
- Hubungan Lama Menjalani Hemodialisa Dengan Tingkat Stres Pada Pasien Gagal Ginjal Kronik Di Rsud Bendan Kota PekalonganDocument6 pagesHubungan Lama Menjalani Hemodialisa Dengan Tingkat Stres Pada Pasien Gagal Ginjal Kronik Di Rsud Bendan Kota PekalonganYuni SumarianiPas encore d'évaluation
- Introduction To Philosophy of The Human Person Quarter 1-Module 5Document24 pagesIntroduction To Philosophy of The Human Person Quarter 1-Module 5Jenelyn BeceraPas encore d'évaluation
- Attest Tech ProfileDocument22 pagesAttest Tech Profileurtical100% (1)
- Approach To Comatose Child: DR G.VenkateshDocument83 pagesApproach To Comatose Child: DR G.VenkateshG VenkateshPas encore d'évaluation
- Inotropes + Electrolyte Imbalance: Presented By: Asya AmeenDocument53 pagesInotropes + Electrolyte Imbalance: Presented By: Asya AmeenAsia AmeenPas encore d'évaluation
- Eusebio v. EusebioDocument4 pagesEusebio v. EusebiosofiaqueenPas encore d'évaluation
- Radiology Presentation FinalDocument45 pagesRadiology Presentation FinalKhupe KafundaPas encore d'évaluation
- Chatper 7. Nursing Care of The Older Adult in Chronic Illness ModuleDocument17 pagesChatper 7. Nursing Care of The Older Adult in Chronic Illness ModuleAriane-Gay Cristobal DuranPas encore d'évaluation
- Tomato Jam Processing GuideDocument4 pagesTomato Jam Processing GuideCandy Concepcion PadizPas encore d'évaluation
- Begonia Rex 06 HiDocument16 pagesBegonia Rex 06 HiDan DanutPas encore d'évaluation
- CPR ChecklistDocument3 pagesCPR ChecklistWan Liyana Naznim57% (7)
- Social SkillS4 Children Teen As PerDocument170 pagesSocial SkillS4 Children Teen As PerFainia Lytra100% (4)
- BioStats AllDocument528 pagesBioStats Allappnu2dwildPas encore d'évaluation
- Study: COVID Booster Effectiveness Wanes But Remains Strong: Credit: Unsplash/CC0 Public DomainDocument2 pagesStudy: COVID Booster Effectiveness Wanes But Remains Strong: Credit: Unsplash/CC0 Public DomainShiny LuNaPas encore d'évaluation
- K to 12 PE Curriculum Guide ExplainedDocument23 pagesK to 12 PE Curriculum Guide ExplainedMelencio Jr BucioPas encore d'évaluation
- Soebandiri Division of Hematology & Medic Oncology Departement of Medicine Airlangga University of MedicineDocument23 pagesSoebandiri Division of Hematology & Medic Oncology Departement of Medicine Airlangga University of MedicineLaura ChandraPas encore d'évaluation
- WHMIS Classification Symbols GuideDocument3 pagesWHMIS Classification Symbols GuideHameed Bin AhmadPas encore d'évaluation
- Amaranthus Spinosus (Kulitis)Document9 pagesAmaranthus Spinosus (Kulitis)sjvpamposa_232360450Pas encore d'évaluation
- ICM Resource Packet 2 Model Curriculum Outline NEWDocument37 pagesICM Resource Packet 2 Model Curriculum Outline NEWMumtihana Muchlis100% (1)
- Chapter2 KnowingOneselfDocument4 pagesChapter2 KnowingOneselfJulieta Lumapas OdtojanPas encore d'évaluation
- PREBORD NLE8part1Document671 pagesPREBORD NLE8part1Bryan NorwaynePas encore d'évaluation
- 1.4 Digestive System in HumanDocument14 pages1.4 Digestive System in HumanNaura RahmaPas encore d'évaluation
- have CB. This difference was statistically significant (p =Relationships among concha bullosa, nasal septal deviation and sinusitisDocument5 pageshave CB. This difference was statistically significant (p =Relationships among concha bullosa, nasal septal deviation and sinusitisandiniPas encore d'évaluation
- Biographical DataDocument2 pagesBiographical DataKenzo WongPas encore d'évaluation
- People's Friendship University of Russia: Acute Odontogenic and Hematogenous OsteomyelitisDocument22 pagesPeople's Friendship University of Russia: Acute Odontogenic and Hematogenous OsteomyelitisAyad IbrahimPas encore d'évaluation
- Breathing - Refining ExerciseDocument8 pagesBreathing - Refining Exercisesachipatel100% (1)