Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- 2011 OctoberDocument11 pages2011 OctoberMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Dengue 208Document3 pagesDengue 208Mohamed Rikarz Ahamed RikarzPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Hypoxemic Respiratory FailureDocument70 pagesHypoxemic Respiratory FailureMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Hemodynamic Changes in Hypotensive Shock: Lcs LumDocument2 pagesHemodynamic Changes in Hypotensive Shock: Lcs LumMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- 12 Kasper Notes 2020 OphthalmologyDocument33 pages12 Kasper Notes 2020 OphthalmologyMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- 643 PDFDocument1 page643 PDFMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- Rheumatology Notes For ReadingDocument8 pagesRheumatology Notes For ReadingMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- 642Document1 page642Mohamed Rikarz Ahamed RikarzPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- 640Document1 page640Mohamed Rikarz Ahamed RikarzPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Dengue 201Document6 pagesDengue 201Mohamed Rikarz Ahamed RikarzPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
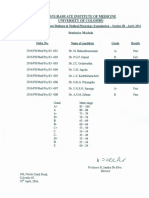
- Results of The Selection Examination in Surgery - .January/February, 2017Document1 pageResults of The Selection Examination in Surgery - .January/February, 2017Mohamed Rikarz Ahamed RikarzPas encore d'évaluation
- Postgraduate Institute of Medicine University of Colombo: 2017/SEIMDIFM - 003Document1 pagePostgraduate Institute of Medicine University of Colombo: 2017/SEIMDIFM - 003Mohamed Rikarz Ahamed RikarzPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Postgraduate Institute of Medicine University of Colombo: Results of The MD (Medicine) Examination-February/March, 2016Document2 pagesPostgraduate Institute of Medicine University of Colombo: Results of The MD (Medicine) Examination-February/March, 2016Mohamed Rikarz Ahamed RikarzPas encore d'évaluation
- Counter Signed: ST THDocument1 pageCounter Signed: ST THMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Postgraduate Nstitute of Med C E University of Colombo: LT S T III A Il, 2016Document1 pagePostgraduate Nstitute of Med C E University of Colombo: LT S T III A Il, 2016Mohamed Rikarz Ahamed RikarzPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Answers To Questions For Volume 11, Number 4: The Surgical Approach To Postpartum HaemorrhageDocument6 pagesAnswers To Questions For Volume 11, Number 4: The Surgical Approach To Postpartum HaemorrhageMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Postgraduate Institute of Medicine University of ColomboDocument1 pagePostgraduate Institute of Medicine University of ColomboMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Checked Counter A: by byDocument1 pageChecked Counter A: by byMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Check dBY - ... - .. By: Counter Signed Ak ExamintuionsDocument1 pageCheck dBY - ... - .. By: Counter Signed Ak ExamintuionsMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Postgraduate Inst Tute of Medici E Universit of ColomboDocument1 pagePostgraduate Inst Tute of Medici E Universit of ColomboMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Postg Aduate Institute of Medicine University FC LomboDocument1 pagePostg Aduate Institute of Medicine University FC LomboMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- Postgraduate Institute of Medicine University of ColomboDocument2 pagesPostgraduate Institute of Medicine University of ColomboMohamed Rikarz Ahamed RikarzPas encore d'évaluation
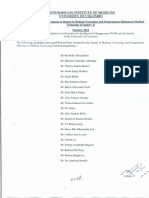
- Postgraduate Institute of Medicine University of Colombo: Index No. Name of CandidateDocument2 pagesPostgraduate Institute of Medicine University of Colombo: Index No. Name of CandidateMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- Postgraduate Institute of Medicine University of ColomboDocument1 pagePostgraduate Institute of Medicine University of ColomboMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- 594 PDFDocument1 page594 PDFMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- Postgraduate Institute of Medicine University of ColomboDocument2 pagesPostgraduate Institute of Medicine University of ColomboMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- Postgraduate Institute of Medicine University of Colombo: (Provisional and SenateDocument1 pagePostgraduate Institute of Medicine University of Colombo: (Provisional and SenateMohamed Rikarz Ahamed RikarzPas encore d'évaluation
- Geographical Milieu of Ancient KashiDocument14 pagesGeographical Milieu of Ancient Kashismk11Pas encore d'évaluation
- PDF Certificacion 3dsmaxDocument2 pagesPDF Certificacion 3dsmaxAriel Carrasco AlmanzaPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Customer AnalysisDocument6 pagesCustomer AnalysisLina LambotPas encore d'évaluation
- Types of CostsDocument9 pagesTypes of CostsPrathna AminPas encore d'évaluation
- Singular & Plural Nouns: Regular PluralsDocument4 pagesSingular & Plural Nouns: Regular PluralsМарина ВетерPas encore d'évaluation
- The Old Man and The SeaDocument6 pagesThe Old Man and The Seahomeless_heartPas encore d'évaluation
- Winifred Breines The Trouble Between Us An Uneasy History of White and Black Women in The Feminist MovementDocument279 pagesWinifred Breines The Trouble Between Us An Uneasy History of White and Black Women in The Feminist MovementOlgaPas encore d'évaluation
- Present Tenses ReviewDocument6 pagesPresent Tenses ReviewRamona DinuPas encore d'évaluation
- Practical Interpretation and Application of Exoc Rine Panc Rea Tic Tes Ting in Small AnimalsDocument20 pagesPractical Interpretation and Application of Exoc Rine Panc Rea Tic Tes Ting in Small Animalsl.fernandagonzalez97Pas encore d'évaluation
- PPG ReviewerDocument8 pagesPPG Reviewerryanbaldoria.immensity.ictPas encore d'évaluation
- Tutorials in Complex Photonic Media SPIE Press Monograph Vol PM194 PDFDocument729 pagesTutorials in Complex Photonic Media SPIE Press Monograph Vol PM194 PDFBadunoniPas encore d'évaluation
- Bibliography of Loyalist Source MaterialDocument205 pagesBibliography of Loyalist Source MaterialNancyPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- English 7 Compare Contrast The People Could Fly Harriet TubmanDocument3 pagesEnglish 7 Compare Contrast The People Could Fly Harriet Tubmanapi-508729334Pas encore d'évaluation
- SiteVisit - Name (Done Excel, Pending CC)Document147 pagesSiteVisit - Name (Done Excel, Pending CC)CK AngPas encore d'évaluation
- CM PhysicalDocument14 pagesCM PhysicalLulu Nur HidayahPas encore d'évaluation
- Project Report On Amazon vs. FlipkartDocument86 pagesProject Report On Amazon vs. FlipkartDimple100% (3)
- Chem31.1 Experiment 2Document28 pagesChem31.1 Experiment 2Mia FernandezPas encore d'évaluation
- Hardy-WeinbergEquilibriumSept2012 002 PDFDocument6 pagesHardy-WeinbergEquilibriumSept2012 002 PDFGuntur FaturachmanPas encore d'évaluation
- The First Step Analysis: 1 Some Important DefinitionsDocument4 pagesThe First Step Analysis: 1 Some Important DefinitionsAdriana Neumann de OliveiraPas encore d'évaluation
- Character Skills Snapshot Sample ItemsDocument2 pagesCharacter Skills Snapshot Sample ItemsCharlie BolnickPas encore d'évaluation
- Technical Report WritingDocument21 pagesTechnical Report WritingMalik JalilPas encore d'évaluation
- Building Brand ArchitectureDocument3 pagesBuilding Brand ArchitectureNeazul Hasan100% (1)
- ESC Cardiomyopathy ClassificationDocument7 pagesESC Cardiomyopathy Classificationvalerius83Pas encore d'évaluation
- RH Control - SeracloneDocument2 pagesRH Control - Seraclonewendys rodriguez, de los santosPas encore d'évaluation
- Endogenic Processes (Erosion and Deposition) : Group 3Document12 pagesEndogenic Processes (Erosion and Deposition) : Group 3Ralph Lawrence C. PagaranPas encore d'évaluation
- Chapter 5, 6Document4 pagesChapter 5, 6anmar ahmedPas encore d'évaluation
- ICT LegalEthical Issue PowerPoint PresentationDocument4 pagesICT LegalEthical Issue PowerPoint PresentationReydan MaravePas encore d'évaluation
- Hanssen, Eirik.Document17 pagesHanssen, Eirik.crazijoePas encore d'évaluation
- Durability Problems of 20 Century Reinforced Concrete Heritage Structures and Their RestorationsDocument120 pagesDurability Problems of 20 Century Reinforced Concrete Heritage Structures and Their RestorationsManjunath ShepurPas encore d'évaluation