Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Lesson Plan On Post Natal ExercisesDocument11 pagesLesson Plan On Post Natal Exercisesvarshasharma0593% (15)
- Student Excursion Consent FormDocument4 pagesStudent Excursion Consent Formapi-276186998Pas encore d'évaluation
- Essential Questions in Paediatrics For MRCPCH v2 PDFDocument208 pagesEssential Questions in Paediatrics For MRCPCH v2 PDFa4aboo100% (11)
- Case Study On Acute PyelonephritisDocument85 pagesCase Study On Acute Pyelonephritissanutulsi100% (23)
- Case ReportDocument11 pagesCase ReportBerhanu DigamoPas encore d'évaluation
- The Administration of Medications I. Speaking 'Administering Medications'Document5 pagesThe Administration of Medications I. Speaking 'Administering Medications'Meri AndaniPas encore d'évaluation
- Beth PRC FormDocument11 pagesBeth PRC FormNev Bryan DapitanPas encore d'évaluation
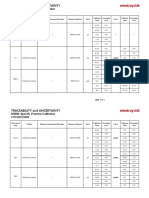
- Specific Proteins Calibrator-150721009-BS600Document2 pagesSpecific Proteins Calibrator-150721009-BS600S6b2Pas encore d'évaluation
- SVTDocument31 pagesSVTAkbar IskandarPas encore d'évaluation
- ShockDocument53 pagesShockHassan Ahmed100% (3)
- Radiologi Gastrointestinal (Noted)Document52 pagesRadiologi Gastrointestinal (Noted)desak 102018084Pas encore d'évaluation
- Needle Prick Injury & PreventionDocument17 pagesNeedle Prick Injury & Preventioniman zainuddinPas encore d'évaluation
- Medication AdministrationDocument8 pagesMedication AdministrationMarku LeePas encore d'évaluation
- EMS Final Exam JulyDocument267 pagesEMS Final Exam Julyraja bouguerraPas encore d'évaluation
- PRE Test 1Document15 pagesPRE Test 1Naomi VirtudazoPas encore d'évaluation
- Surgical Management of Gastroesophageal Reflux in Adults - UpToDateDocument22 pagesSurgical Management of Gastroesophageal Reflux in Adults - UpToDateJuan InsignaresPas encore d'évaluation
- Parameters of The Model: Name Live Alpha Beta DescriptionDocument5 pagesParameters of The Model: Name Live Alpha Beta DescriptionAngga Prawira KautsarPas encore d'évaluation
- Vitamin and Mineral Supplementation During PregnanDocument4 pagesVitamin and Mineral Supplementation During PregnanEvi RachmawatiPas encore d'évaluation
- An Unconscious Patient With A DNR TattooDocument2 pagesAn Unconscious Patient With A DNR TattoonadaPas encore d'évaluation
- Hospital Outpatient Prospective Payment System 2019 Updates - Shared1Document112 pagesHospital Outpatient Prospective Payment System 2019 Updates - Shared1Nunya BiznesPas encore d'évaluation
- Is Doa 10 Cup TestDocument1 pageIs Doa 10 Cup TestUqi.Pas encore d'évaluation
- Comorbidity: Apakah Merupakan Faktor Risiko: Infeksi Luka Operasi Pasca Seksio Sesarea?Document10 pagesComorbidity: Apakah Merupakan Faktor Risiko: Infeksi Luka Operasi Pasca Seksio Sesarea?Dini AgustiniPas encore d'évaluation
- BIO 211 Chapter 18 AssignmentDocument20 pagesBIO 211 Chapter 18 Assignmentf1l2o3r4e5n6Pas encore d'évaluation
- 103, Kanakia - B. Zillion Building, Lbs Marg, Kurla (W), Mumbai - 400 070Document10 pages103, Kanakia - B. Zillion Building, Lbs Marg, Kurla (W), Mumbai - 400 0708460074686Pas encore d'évaluation
- Braden ScaleDocument1 pageBraden ScaleRandall StevensPas encore d'évaluation
- Shellfish AllergyDocument23 pagesShellfish AllergyThessa Vee Capuno RioPas encore d'évaluation
- Travatan (Travoprost Ophthalmic Solution) 0.004% SterileDocument7 pagesTravatan (Travoprost Ophthalmic Solution) 0.004% SterileSyed Shariq AliPas encore d'évaluation
- Hypopyon in Acute Lymphoblastic Leukemia A Case ReportDocument2 pagesHypopyon in Acute Lymphoblastic Leukemia A Case ReportInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Operative ProcedureDocument22 pagesOperative Procedurezianab aliPas encore d'évaluation
- IDP 11.13.19 11.14.19 Metal Implants White Paper - 0 PDFDocument152 pagesIDP 11.13.19 11.14.19 Metal Implants White Paper - 0 PDFVivek KhakharPas encore d'évaluation