Vous aimerez peut-être aussi
- Adrenal Gland: DR - Sabri.S.EltayebDocument53 pagesAdrenal Gland: DR - Sabri.S.EltayebhamidPas encore d'évaluation
- Urinary System: Cytology, Histology, Cystoscopy, and RadiologyD'EverandUrinary System: Cytology, Histology, Cystoscopy, and RadiologyPas encore d'évaluation
- Acute PancreatitisDocument46 pagesAcute PancreatitisLew NianPas encore d'évaluation
- Jaundice: DR: Ramy A. SamyDocument42 pagesJaundice: DR: Ramy A. Samyoscar3spurgeonPas encore d'évaluation
- Urinary Tract CalculiDocument34 pagesUrinary Tract CalculiOnkar SinghPas encore d'évaluation
- Peripheral Arterial DiseaseDocument5 pagesPeripheral Arterial Diseaseampogison08Pas encore d'évaluation
- JaundiceDocument53 pagesJaundiceAbhishiktaAbhiPas encore d'évaluation
- Vascular Diseases (1 of 3)Document4 pagesVascular Diseases (1 of 3)Doctor GeneralPas encore d'évaluation
- Small - Intestinal Neoplasms and Carcinoid TumorsDocument51 pagesSmall - Intestinal Neoplasms and Carcinoid TumorsOlga GoryachevaPas encore d'évaluation
- 7 - The Biliary TractDocument48 pages7 - The Biliary TractKim RamosPas encore d'évaluation
- Akut AbdomenDocument38 pagesAkut AbdomenAprianPas encore d'évaluation
- Case Presentation Lump Right HypochondriumDocument22 pagesCase Presentation Lump Right HypochondriumNANDAN RAIPas encore d'évaluation
- Acute AbdomenDocument122 pagesAcute AbdomenJunayed Safar MahmudPas encore d'évaluation
- Anatomy of Circulatory SystemDocument56 pagesAnatomy of Circulatory SystemLina Wijaya100% (1)
- Acute Pain Abdomen in Surgical PracticeDocument34 pagesAcute Pain Abdomen in Surgical PracticedrakashnardePas encore d'évaluation
- Surgical Diseases of The EsophagusDocument35 pagesSurgical Diseases of The Esophagusmogesie1995Pas encore d'évaluation
- CSF AnalysisDocument6 pagesCSF Analysisfrederico_Pas encore d'évaluation
- General Surgery SMALL INTESTINES-Dr MendozaDocument101 pagesGeneral Surgery SMALL INTESTINES-Dr MendozaMedisina101Pas encore d'évaluation
- 01 - Signs and Symptoms of Git DisordersDocument51 pages01 - Signs and Symptoms of Git DisordersRere AnugrahPas encore d'évaluation
- Physiology of The Gastrointestinal Tract (Git)Document98 pagesPhysiology of The Gastrointestinal Tract (Git)jballungayPas encore d'évaluation
- Investigation and Treatment of Surgical JaundiceDocument38 pagesInvestigation and Treatment of Surgical JaundiceUjas PatelPas encore d'évaluation
- Lecture: Adrenal DisordersDocument78 pagesLecture: Adrenal DisordersOchendo KingxPas encore d'évaluation
- Hepato-Biliary System 26.4.2016Document59 pagesHepato-Biliary System 26.4.2016S B SayedPas encore d'évaluation
- Inguinal Hernias and Abdominal Wall Defects: Murad Nuserat & Abd AL-Rahman AlhelwDocument51 pagesInguinal Hernias and Abdominal Wall Defects: Murad Nuserat & Abd AL-Rahman AlhelwRashed ShatnawiPas encore d'évaluation
- Parathyroid Glands: Presented By: Dr. Mohammed Alshehri Pgy2Document28 pagesParathyroid Glands: Presented By: Dr. Mohammed Alshehri Pgy2Omar Alruwaili100% (1)
- GoitreDocument6 pagesGoitreJohn Vladimir A. BulagsayPas encore d'évaluation
- N196 GI Exam Study GuideDocument7 pagesN196 GI Exam Study Guideaznknight3230% (1)
- Pancreas Pancreatic DisordersDocument48 pagesPancreas Pancreatic DisordersAmjad NiaziPas encore d'évaluation
- Acute AbdomenDocument8 pagesAcute Abdomenarum1992Pas encore d'évaluation
- Carcinoma Pancreas: Risk Factors: (A) Demographic FactorsDocument4 pagesCarcinoma Pancreas: Risk Factors: (A) Demographic FactorsSakthi Annamalai.cPas encore d'évaluation
- Clinical Science Section Acute Abdomen: Preseptor: Dr. Liza Nursanty, SPB, Mkes, FinacsDocument40 pagesClinical Science Section Acute Abdomen: Preseptor: Dr. Liza Nursanty, SPB, Mkes, FinacsPraluki HerliawanPas encore d'évaluation
- Kidney StonesDocument65 pagesKidney StonesnazmiPas encore d'évaluation
- Obstructive Uropathy PDFDocument83 pagesObstructive Uropathy PDFAfrizal Adz100% (1)
- 10 EdemaDocument23 pages10 EdemaTalmaciu AmyPas encore d'évaluation
- PeritonitisDocument34 pagesPeritonitisabrar_zaidiPas encore d'évaluation
- Differential Diagnosis Pain Right HypochondriumDocument35 pagesDifferential Diagnosis Pain Right HypochondriumDrArish Mahmood100% (1)
- Paeds Crack Notes-1Document111 pagesPaeds Crack Notes-1Ashutosh Krishna JadhavPas encore d'évaluation
- Anatomy of EsophagusDocument18 pagesAnatomy of Esophagusgabbyneng0% (1)
- Acute Coronary Syndrome: Rich Derby, LT Col, USAF MGMC Family Practice ProgramDocument56 pagesAcute Coronary Syndrome: Rich Derby, LT Col, USAF MGMC Family Practice ProgramprincezastaridaPas encore d'évaluation
- GangrenDocument3 pagesGangrenBurhan uddinPas encore d'évaluation
- Bio StatisticsDocument122 pagesBio StatisticsSweta SaravananPas encore d'évaluation
- Peptic Ulcers: DR Yotham Phiri Mmed (Surg)Document46 pagesPeptic Ulcers: DR Yotham Phiri Mmed (Surg)Emmanuel MukukaPas encore d'évaluation
- SepsisDocument33 pagesSepsisv_vijayakanth7656Pas encore d'évaluation
- HypertensionDocument12 pagesHypertensionDr. PARMINDER NAINPas encore d'évaluation
- Urological EmergencyDocument83 pagesUrological EmergencyAlfred LiPas encore d'évaluation
- Anatomy of Thyroid GlandDocument12 pagesAnatomy of Thyroid GlandBinbinbabu BinuPas encore d'évaluation
- Radiology of The Urinary SystemDocument78 pagesRadiology of The Urinary Systemapi-19916399Pas encore d'évaluation
- Renovascular Hypertension (RVH) SeminarDocument58 pagesRenovascular Hypertension (RVH) SeminarfaizalmasoodiPas encore d'évaluation
- Perianal Problems: ACS/ASE Medical Student Core Curriculum Perianal ProblemsDocument21 pagesPerianal Problems: ACS/ASE Medical Student Core Curriculum Perianal ProblemsHasti Chande100% (1)
- Differential Diagnosis of A Renal MassDocument23 pagesDifferential Diagnosis of A Renal Massmdjohari100% (1)
- Scrotal SwellingDocument123 pagesScrotal SwellingLestari Amelia AdmPas encore d'évaluation
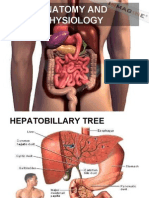
- Anatomy and PhysiologyDocument24 pagesAnatomy and PhysiologyGillarhymesPas encore d'évaluation
- Cushing DiseaseDocument24 pagesCushing DiseaseSuci AlimaPas encore d'évaluation
- Arterial InsufficiencyDocument48 pagesArterial InsufficiencySyAmil MeNzaPas encore d'évaluation
- Introduction To The Topographical Anatomy and Operative SurgeryDocument43 pagesIntroduction To The Topographical Anatomy and Operative SurgeryKavan Vyas100% (1)
- Inflammatory Bowel DiseaseDocument51 pagesInflammatory Bowel DiseaseTeena Chandran100% (1)
- 58 Lower Gastrointestinal BleedDocument4 pages58 Lower Gastrointestinal BleedLuphly TaluvtaPas encore d'évaluation
- 54.the Gallbladder and Bile DuctsDocument19 pages54.the Gallbladder and Bile DuctsAdenegan Adesola RaymondPas encore d'évaluation
- Chest and Abdominal Injuries: Forensic Medicine by Yazan AbueidehDocument54 pagesChest and Abdominal Injuries: Forensic Medicine by Yazan AbueidehRayyan Alali100% (1)
- Female Reproductive Organ 2016Document8 pagesFemale Reproductive Organ 2016Nabilah Armalia IffahPas encore d'évaluation
- Anatomy of Female PelvicDocument34 pagesAnatomy of Female PelvicNabilah Armalia IffahPas encore d'évaluation
- Abnormal Uterine BleedingDocument19 pagesAbnormal Uterine BleedingNabilah Armalia IffahPas encore d'évaluation
- STUDENT Motion+SicknessDocument20 pagesSTUDENT Motion+SicknessNabilah Armalia IffahPas encore d'évaluation
- STUDENT Motion+SicknessDocument21 pagesSTUDENT Motion+SicknessNabilah Armalia IffahPas encore d'évaluation
- Organ-Organ Limfoid: Thymus Dan LimfonodusDocument9 pagesOrgan-Organ Limfoid: Thymus Dan LimfonodusNabilah Armalia IffahPas encore d'évaluation
- Motion SicknessDocument23 pagesMotion SicknessNabilah Armalia IffahPas encore d'évaluation
- The Musculoskeletal SystemDocument44 pagesThe Musculoskeletal SystemNabilah Armalia IffahPas encore d'évaluation
- IntussusceptionDocument24 pagesIntussusceptionOjambo Flavia100% (1)
- KODINGDocument5 pagesKODINGDesy RusianaPas encore d'évaluation
- L28 - Esophageal DiseasesDocument16 pagesL28 - Esophageal DiseasesNimer Abdelhadi AliPas encore d'évaluation
- Esophagus 1Document39 pagesEsophagus 1Yousif Ahmed DAPas encore d'évaluation
- CholelithiasisDocument6 pagesCholelithiasisLara GatbontonPas encore d'évaluation
- Primary Biliary CirrhosisDocument8 pagesPrimary Biliary CirrhosisAhmed TeebiPas encore d'évaluation
- Daftar Pustaka Refarat RadiologiDocument6 pagesDaftar Pustaka Refarat RadiologiOvelin LarasatiPas encore d'évaluation
- 12 - Paediatric Abdomen RadiologyDocument74 pages12 - Paediatric Abdomen RadiologyMaria DoukaPas encore d'évaluation
- GastritisDocument10 pagesGastritisMario100% (2)
- Pathophysiology of HemorrhoidsDocument2 pagesPathophysiology of HemorrhoidsTrixie FayePas encore d'évaluation
- 4 Stages of Cirrhosis of The Liver 18 Symptoms, CDocument9 pages4 Stages of Cirrhosis of The Liver 18 Symptoms, CRammy KhanPas encore d'évaluation
- Report JaundiceDocument2 pagesReport JaundiceVishal KumarPas encore d'évaluation
- Seminar Power PointDocument20 pagesSeminar Power PointNoor KhaiatPas encore d'évaluation
- ENEMADocument16 pagesENEMAoxidalaj100% (8)
- Management of Cirrhosis of The LiverDocument48 pagesManagement of Cirrhosis of The LiverksofianaPas encore d'évaluation
- Acute and Chronic Gastrointestinal BleedingDocument7 pagesAcute and Chronic Gastrointestinal BleedingMarwan M.100% (1)
- DAFTAR PUSTAKA JokoDocument2 pagesDAFTAR PUSTAKA JokoDoctor's BettaPas encore d'évaluation
- ILEUS.,,... Kuliah Internasional Prof MTDocument10 pagesILEUS.,,... Kuliah Internasional Prof MTtatadhPas encore d'évaluation
- Assess BowelDocument2 pagesAssess BowelneoclintPas encore d'évaluation
- 2012 Complete Board Questions PDFDocument43 pages2012 Complete Board Questions PDFbmhshPas encore d'évaluation
- Esophagitis: Laura Nevaranda 1610211088Document32 pagesEsophagitis: Laura Nevaranda 1610211088Qara Syifa FPas encore d'évaluation
- CASE PRESENTATION OF Obstructive JaundiceDocument25 pagesCASE PRESENTATION OF Obstructive JaundiceKhalid RizwanPas encore d'évaluation
- Gallbladder DisordersDocument59 pagesGallbladder DisordersdrelvPas encore d'évaluation
- 1 Small and Large Intestine DisordersDocument44 pages1 Small and Large Intestine DisordersSirat KhanPas encore d'évaluation
- Epidemiology, Clinical Characteristics, and Treatment of Children With Acute Intussusception: A Case SeriesDocument6 pagesEpidemiology, Clinical Characteristics, and Treatment of Children With Acute Intussusception: A Case SeriesIqbal RifaiPas encore d'évaluation
- Comparison of Endoscopic and Surgical Treatment For Acute Cholangitis Caused by CholedocolithiasisDocument12 pagesComparison of Endoscopic and Surgical Treatment For Acute Cholangitis Caused by CholedocolithiasismonchoellesPas encore d'évaluation
- Cholecystitis BelgradeDocument52 pagesCholecystitis BelgradeLazar VučetićPas encore d'évaluation
- Liver Cirrhosis: Dr. Soegiarto Gani, SPPDDocument26 pagesLiver Cirrhosis: Dr. Soegiarto Gani, SPPDmirwan bakriPas encore d'évaluation
- Causes of Upper Gastrointestinal Bleeding in Adults UpToDateDocument37 pagesCauses of Upper Gastrointestinal Bleeding in Adults UpToDateJodene Rose RojasPas encore d'évaluation
- Bowel ObstructionDocument46 pagesBowel ObstructionAhmadNurwanto100% (1)