Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Disease and DefenceDocument5 pagesDisease and DefenceNabindra Ruwali100% (1)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Fundamental Principles of Human Anatomy & Physiology: July 2016Document41 pagesFundamental Principles of Human Anatomy & Physiology: July 2016mabel yapuraPas encore d'évaluation
- 1 - Anatomy of The KidneyDocument15 pages1 - Anatomy of The Kidneysara khanPas encore d'évaluation
- Case Study (Bronchial Asthma)Document11 pagesCase Study (Bronchial Asthma)DhanNie Cenita50% (2)
- The Digestive System LabelDocument3 pagesThe Digestive System LabelUSMP FN ARCHIVOSPas encore d'évaluation
- Ilovepdf MergedDocument457 pagesIlovepdf MergedMar LoyolaPas encore d'évaluation
- EmbryologyDocument68 pagesEmbryologyBj Larracas100% (1)
- Autoimmune Disease MechanismsDocument6 pagesAutoimmune Disease MechanismsHaliunaa BattulgaPas encore d'évaluation
- Summative Exam 4thDocument48 pagesSummative Exam 4thJohn Van Dave Taturo100% (1)
- Testicular Torsion: Dr. Hari Krismanuel, Sp. B, FinacsDocument19 pagesTesticular Torsion: Dr. Hari Krismanuel, Sp. B, FinacsVanessa Modi AlverinaPas encore d'évaluation
- Hamartomas of Mature Cardiac Myocytes: Report of 7 New Cases and Review of LiteratureDocument8 pagesHamartomas of Mature Cardiac Myocytes: Report of 7 New Cases and Review of LiteratureAntonio FgPas encore d'évaluation
- Cardiactumors: Dylan V. MillerDocument31 pagesCardiactumors: Dylan V. MillerAntonio FgPas encore d'évaluation
- Pulmonary Pathology and COVID-19Document14 pagesPulmonary Pathology and COVID-19Antonio FgPas encore d'évaluation
- Historia Natural de La Fibrosis PulmonarDocument8 pagesHistoria Natural de La Fibrosis PulmonarAntonio FgPas encore d'évaluation
- Tumours of The Heart. W.H.O. 2004 3rd EditionDocument40 pagesTumours of The Heart. W.H.O. 2004 3rd EditionAntonio FgPas encore d'évaluation
- Figo Staging Systems 2009Document31 pagesFigo Staging Systems 2009Antonio FgPas encore d'évaluation
- Foetal Membrane and Amniotic Fluid FunctionsDocument10 pagesFoetal Membrane and Amniotic Fluid FunctionsN. SivaPas encore d'évaluation
- DedeDocument8 pagesDedeHannah V. LacambraPas encore d'évaluation
- Neuroanatomy Notes for Neuropsychology ClassDocument35 pagesNeuroanatomy Notes for Neuropsychology ClassBetsabé VZPas encore d'évaluation
- MH Introduction To HistologyDocument46 pagesMH Introduction To HistologyFefê BrittoPas encore d'évaluation
- Activity No. 7.1 BloodDocument2 pagesActivity No. 7.1 BloodDree SermanPas encore d'évaluation
- 29.3 Book BioDocument4 pages29.3 Book BioBadawi ashrafPas encore d'évaluation
- Harrison's Review - Chapter 65 Bleeding and ThrombosisDocument2 pagesHarrison's Review - Chapter 65 Bleeding and ThrombosisJason CentenoPas encore d'évaluation
- ANATOMY Final Spots 205Document2 pagesANATOMY Final Spots 205anojanPas encore d'évaluation
- What living things are made of cells, tissues, organs and systemsDocument10 pagesWhat living things are made of cells, tissues, organs and systemsRamyRamia ElzantPas encore d'évaluation
- Bone HealingDocument7 pagesBone HealingArfan PrawiragaraPas encore d'évaluation
- Cell Fractionation & Marker EnzymesDocument20 pagesCell Fractionation & Marker EnzymesVivek PPas encore d'évaluation
- Vomiting Dog Yellow - Google SearchDocument1 pageVomiting Dog Yellow - Google SearchCLIFFORD JUANPas encore d'évaluation
- Animal Tissues WorksheetDocument8 pagesAnimal Tissues WorksheetMaxene LuisPas encore d'évaluation
- The Effect of Drugs On CNSDocument2 pagesThe Effect of Drugs On CNShaydenchiaPas encore d'évaluation
- Anemia and Critical CareDocument77 pagesAnemia and Critical Carehunter_axl010% (1)
- Cutaneous CirculationDocument19 pagesCutaneous CirculationShubhamPas encore d'évaluation
- Year 4 Reading Your Digestive SystemDocument11 pagesYear 4 Reading Your Digestive SystemMa Donabel LopezPas encore d'évaluation
- Grade 4 Summative Test for Science and Music Covers Key ConceptsDocument2 pagesGrade 4 Summative Test for Science and Music Covers Key ConceptsCristita Macaranas Vigo100% (1)
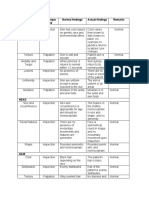
- Area Assessed Technique Used Normal Findings Actual Findings Remarks SkinDocument6 pagesArea Assessed Technique Used Normal Findings Actual Findings Remarks SkinLadybelle GototosPas encore d'évaluation
- Fine Needle Aspiration Cytology (FNAC) of GISTDocument7 pagesFine Needle Aspiration Cytology (FNAC) of GISTurfriendanshul100% (1)