Vous aimerez peut-être aussi
- Acs Risk Stratification and Clinical ManagementDocument41 pagesAcs Risk Stratification and Clinical ManagementannisPas encore d'évaluation
- Cardiac Risk AssessmentDocument4 pagesCardiac Risk Assessmentmonir61Pas encore d'évaluation
- Ing 5Document11 pagesIng 5Farida MufidatiPas encore d'évaluation
- Peripartum Cardiomyopathy: From Pathophysiology to ManagementD'EverandPeripartum Cardiomyopathy: From Pathophysiology to ManagementPas encore d'évaluation
- Wang Et Al - Older Age and Outcome AfterDocument9 pagesWang Et Al - Older Age and Outcome AfterMurat MukharyamovPas encore d'évaluation
- 62 Full PDFDocument12 pages62 Full PDFrizkiaautikasariPas encore d'évaluation
- MayoclinprocDocument12 pagesMayoclinprocpriyaPas encore d'évaluation
- Becattini 2018Document25 pagesBecattini 2018Snezana MihajlovicPas encore d'évaluation
- Coronary Vasomotion AbnormalitiesD'EverandCoronary Vasomotion AbnormalitiesHiroaki ShimokawaPas encore d'évaluation
- Coronary Calcium: A Comprehensive Understanding of Its Biology, Use in Screening, and Interventional ManagementD'EverandCoronary Calcium: A Comprehensive Understanding of Its Biology, Use in Screening, and Interventional ManagementAloke Virmani FinnPas encore d'évaluation
- Rationale and Design of The Coronary Computed Tomographic Angiography For Selective Cardiac CatheterizationDocument9 pagesRationale and Design of The Coronary Computed Tomographic Angiography For Selective Cardiac Catheterizationganda gandaPas encore d'évaluation
- CPG Unstable AnginaDocument58 pagesCPG Unstable AnginaAmir HassenPas encore d'évaluation
- Dzudie 2020Document7 pagesDzudie 2020Andi Tiara S. AdamPas encore d'évaluation
- Heart J: Outcome of Primary Percutaneous Coronary Intervention With Early and Late ST Resolution - Earlier Is Better!Document6 pagesHeart J: Outcome of Primary Percutaneous Coronary Intervention With Early and Late ST Resolution - Earlier Is Better!ayesha FalakPas encore d'évaluation
- CRM ResidHighGradeangina2007Document5 pagesCRM ResidHighGradeangina2007Aryadhi TevataqsaPas encore d'évaluation
- Clinical characteristics and outcomes of STEMI patients in Bali, IndonesiaDocument10 pagesClinical characteristics and outcomes of STEMI patients in Bali, IndonesiaDavy JonesPas encore d'évaluation
- Rajiv Gandhi University of Health Sciences, Bangalore, KarnatakaDocument18 pagesRajiv Gandhi University of Health Sciences, Bangalore, KarnatakaprashantghodkePas encore d'évaluation
- Cardioversion of Atrial Fibrillation in Obese Patients: Results From The Cardioversion-BMI Randomized Controlled TrialDocument22 pagesCardioversion of Atrial Fibrillation in Obese Patients: Results From The Cardioversion-BMI Randomized Controlled TrialAttilio Del RossoPas encore d'évaluation
- Management of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)D'EverandManagement of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)Pas encore d'évaluation
- The Management of Patients With Acute Myocardial Infarction: Pocket GuidelinesDocument21 pagesThe Management of Patients With Acute Myocardial Infarction: Pocket GuidelinesRubelyn Joy LazartePas encore d'évaluation
- ECMO: An Overview of Lung and Heart SupportDocument133 pagesECMO: An Overview of Lung and Heart SupportrisanataliasiburianPas encore d'évaluation
- Guidelines of Implementation For The Management of Acs Focus On Coronary InterventionDocument33 pagesGuidelines of Implementation For The Management of Acs Focus On Coronary InterventionannisPas encore d'évaluation
- CARDIAC EMERGENCIES IN DAILY PRACTICEDocument45 pagesCARDIAC EMERGENCIES IN DAILY PRACTICEnikenPas encore d'évaluation
- Randomized Trial of Stents Versus Bypass Surgery For Left Main Coronary Artery DiseaseDocument9 pagesRandomized Trial of Stents Versus Bypass Surgery For Left Main Coronary Artery DiseaseTommy WidjayaPas encore d'évaluation
- Yamamoto Et Al 2019 Clinical and Laboratory Predictors For Plaque Erosion in Patients With Acute Coronary SyndromesDocument18 pagesYamamoto Et Al 2019 Clinical and Laboratory Predictors For Plaque Erosion in Patients With Acute Coronary SyndromesMarcellia AngelinaPas encore d'évaluation
- 26 PDFDocument5 pages26 PDFBaru Chandrasekhar RaoPas encore d'évaluation
- PIIS1078588419310755Document7 pagesPIIS1078588419310755zeeshan qurbanPas encore d'évaluation
- CABG Surgical Case Study EditeDocument18 pagesCABG Surgical Case Study Editemaduwanthaharsha88Pas encore d'évaluation
- ER Case SofanDocument46 pagesER Case SofanDavid JonathanPas encore d'évaluation
- Aortic Valve Disease Guidelines PDFDocument36 pagesAortic Valve Disease Guidelines PDFStefan Marev GerganovPas encore d'évaluation
- Jurnal 1 GadarDocument6 pagesJurnal 1 GadarDwi FebriyantiPas encore d'évaluation
- Retired Firefighter of 40 Years Grateful For The Help of Doctors at HCA Florida MemorialDocument9 pagesRetired Firefighter of 40 Years Grateful For The Help of Doctors at HCA Florida MemorialSarah GlennPas encore d'évaluation
- The Shortfall in Long-Term Survival of Patients With Repaired Thoracic Orabdominal Aortic Aneurysms Retrospective CaseeControl Analysis Ofhospital Episode StatisticsDocument9 pagesThe Shortfall in Long-Term Survival of Patients With Repaired Thoracic Orabdominal Aortic Aneurysms Retrospective CaseeControl Analysis Ofhospital Episode StatisticsJeffery TaylorPas encore d'évaluation
- Cardiac Monitoring and ECG lesson planDocument8 pagesCardiac Monitoring and ECG lesson planIshfaq RatherPas encore d'évaluation
- Critical (17-24)Document15 pagesCritical (17-24)kololll lllknPas encore d'évaluation
- Cardiac Rehabilitation and Survival in A LargeDocument10 pagesCardiac Rehabilitation and Survival in A LargeGabriela Rodríguez CanitrotPas encore d'évaluation
- 1 Pag 4Document10 pages1 Pag 4Mr. LPas encore d'évaluation
- 1 s2.0 S0914508719303648 MainDocument6 pages1 s2.0 S0914508719303648 MainMarina UlfaPas encore d'évaluation
- Full RevascDocument10 pagesFull RevascfelipePas encore d'évaluation
- The Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsDocument5 pagesThe Importance of Mean Platelet Volume To Lymphocyte Ratio in Predicting Atrial Fibrillation After Coronary Bypass OperationsM Ali AdrianPas encore d'évaluation
- Cardiology Update 2018 The First QuarterDocument6 pagesCardiology Update 2018 The First QuarterAditya SutarPas encore d'évaluation
- Ischemic 19Document8 pagesIschemic 19Adina Alexandra CPas encore d'évaluation
- 1952Document4 pages1952Lee Eun HyePas encore d'évaluation
- Cardiac MRI in Diagnosis, Clinical Management, and Prognosis of Arrhythmogenic Right Ventricular Cardiomyopathy/DysplasiaD'EverandCardiac MRI in Diagnosis, Clinical Management, and Prognosis of Arrhythmogenic Right Ventricular Cardiomyopathy/DysplasiaÉvaluation : 5 sur 5 étoiles5/5 (1)
- Percutaneous Transluminal Coronary Angioplasty (PTCA) and Stenting - Study of 100 CasesDocument7 pagesPercutaneous Transluminal Coronary Angioplasty (PTCA) and Stenting - Study of 100 CasesLuqy Luqman EffendyPas encore d'évaluation
- Jos 2019 00024Document13 pagesJos 2019 00024Ainul NurrahmahPas encore d'évaluation
- Oncology Pioneer CVDocument2 pagesOncology Pioneer CVDelureanu SanzianaPas encore d'évaluation
- ADAPT TrialDocument8 pagesADAPT TrialDiego CamposPas encore d'évaluation
- 2022 Care PlanDocument8 pages2022 Care Planapi-601587526Pas encore d'évaluation
- 2021 Jcva Sevrare EcmoDocument13 pages2021 Jcva Sevrare EcmoMiky DinuPas encore d'évaluation
- Computed-Tomography a Powerful Tool for Diagnosis of Pediatric and Adult Congenital Heart Disease: Methodology and Interpretation GuideD'EverandComputed-Tomography a Powerful Tool for Diagnosis of Pediatric and Adult Congenital Heart Disease: Methodology and Interpretation GuidePas encore d'évaluation
- Atualização de Síncope CCS 2020Document11 pagesAtualização de Síncope CCS 2020Carlos RenatoPas encore d'évaluation
- J Interven Cardiol. 2017 1-7.: Presented By: Dr. Yusrina BR Saragih Supervisor: DR - Dr. Zulfikri Mukhtar, Sp. JP (K)Document24 pagesJ Interven Cardiol. 2017 1-7.: Presented By: Dr. Yusrina BR Saragih Supervisor: DR - Dr. Zulfikri Mukhtar, Sp. JP (K)Yusrina Njoes SaragihPas encore d'évaluation
- A Randomized Controlled Trial CCMDocument10 pagesA Randomized Controlled Trial CCMAnonymous NeRC5JYiSPas encore d'évaluation
- Zhao 2020Document8 pagesZhao 2020Moom TakohPas encore d'évaluation
- PIIS1053077021007862Document20 pagesPIIS1053077021007862RicardoPas encore d'évaluation
- Diagnostic Value of Three Dimensional EchocardiogrDocument3 pagesDiagnostic Value of Three Dimensional EchocardiogrAmilkar VazquezPas encore d'évaluation
- Jurnal 3Document8 pagesJurnal 3Alda AdeliaPas encore d'évaluation
- KDIGO Dialysis Initiation Conf Report in PressDocument11 pagesKDIGO Dialysis Initiation Conf Report in PressDesi HutapeaPas encore d'évaluation
- Hyperkalemia: Clinical Update OnDocument4 pagesHyperkalemia: Clinical Update OnHunter Japon TorquiPas encore d'évaluation
- Primary Dislocation of Shoulder in Young PatientDocument8 pagesPrimary Dislocation of Shoulder in Young PatientVivi Anggelia AngPas encore d'évaluation
- Glycemic ControlDocument40 pagesGlycemic ControlVivi Anggelia AngPas encore d'évaluation
- Endometriosis-Associated Ovarian Cancer PDFDocument13 pagesEndometriosis-Associated Ovarian Cancer PDFVivi Anggelia AngPas encore d'évaluation
- CME Prolonged FeverDocument29 pagesCME Prolonged FeverVivi Anggelia AngPas encore d'évaluation
- Global Initiative For COPDDocument44 pagesGlobal Initiative For COPDsajid_saiyadPas encore d'évaluation
- New THT JournalDocument25 pagesNew THT JournalVivi Anggelia AngPas encore d'évaluation
- Perforated Peptic Ulcer Symptoms and DiagnosisDocument68 pagesPerforated Peptic Ulcer Symptoms and DiagnosisSaibo BoldsaikhanPas encore d'évaluation
- Biomarker VulnerabilityDocument3 pagesBiomarker VulnerabilityVivi Anggelia AngPas encore d'évaluation
- The Effect of Include CRPDocument11 pagesThe Effect of Include CRPVivi Anggelia AngPas encore d'évaluation
- Grade 7 Science Summary - The Circulatory SystemDocument10 pagesGrade 7 Science Summary - The Circulatory SystemNadine Salah El-DinPas encore d'évaluation
- Pharm D (PB) 2 YEAR 2020-2021: Under The Guidance of GuideDocument41 pagesPharm D (PB) 2 YEAR 2020-2021: Under The Guidance of Guidesufiya fatimaPas encore d'évaluation
- Placental Growth and Maturation: A Concise OverviewDocument6 pagesPlacental Growth and Maturation: A Concise OverviewClyde Yuchengco Cu-unjiengPas encore d'évaluation
- Bab 2 Ting 1 SainsDocument18 pagesBab 2 Ting 1 SainsbrownsofaPas encore d'évaluation
- SIM 6 Circulatory SystemDocument1 pageSIM 6 Circulatory SystemJelly Flores100% (1)
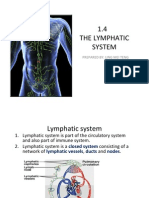
- 1.4 The Lymphatic System: Prepared By: Ling Mei TengDocument15 pages1.4 The Lymphatic System: Prepared By: Ling Mei TengJuliet LingPas encore d'évaluation
- Pediatric Cardiology PDFDocument382 pagesPediatric Cardiology PDFfarzadfusion100% (5)
- Human Physiology in An Aquatic EnvironmentDocument47 pagesHuman Physiology in An Aquatic EnvironmentMARIA CAMILA RENGIFO CAICEDOPas encore d'évaluation
- Hypertensive Vascular DiseaseDocument5 pagesHypertensive Vascular DiseaseGenoMacaraanPas encore d'évaluation
- FloTrac Sensor Clinical UtilityDocument21 pagesFloTrac Sensor Clinical UtilityAnestesia 2017 UDECPas encore d'évaluation
- Anatomy and Physiology of Farm AnimalsDocument157 pagesAnatomy and Physiology of Farm AnimalsOliver Talip100% (1)
- Chapter 8 Transport in Mammals - WorksheetDocument5 pagesChapter 8 Transport in Mammals - Worksheetapi-3728508100% (2)
- Pulmonary Hypertension and Cor PulmonaleDocument93 pagesPulmonary Hypertension and Cor Pulmonalesanjivdas100% (1)
- Anatomy and Physiology: Placement: First YearDocument12 pagesAnatomy and Physiology: Placement: First YearJerin CyriacPas encore d'évaluation
- Exercise 7.2 - ElectrocardiogramDocument2 pagesExercise 7.2 - ElectrocardiogramKevin F. CortesPas encore d'évaluation
- Structure of Blood Vessels - StationsDocument6 pagesStructure of Blood Vessels - StationsRamya MalariniPas encore d'évaluation
- Electrophysiology of HeartDocument46 pagesElectrophysiology of HearthafizahhoshniPas encore d'évaluation
- The Physiology of Cardiopulmonary Resuscitation (CPR) - ECG & ECHODocument9 pagesThe Physiology of Cardiopulmonary Resuscitation (CPR) - ECG & ECHOUrgencias La RazaPas encore d'évaluation
- Proper Vital Signs AssessmentDocument51 pagesProper Vital Signs Assessmentpelly3190100% (2)
- Care of Mother and Child at Risk or With ProblemsDocument87 pagesCare of Mother and Child at Risk or With ProblemsQueen Jyil100% (1)
- Acute Bioligic CrisisDocument141 pagesAcute Bioligic CrisisJanelle MatamorosaPas encore d'évaluation
- Echo Guidelines For Chamber QuantificationDocument24 pagesEcho Guidelines For Chamber QuantificationOnon EssayedPas encore d'évaluation
- Taking Care of the Respiratory and Circulatory SystemsDocument1 pageTaking Care of the Respiratory and Circulatory SystemsKenshin MedinaPas encore d'évaluation
- Cucci Linfedema Generalidades AnatomiaDocument8 pagesCucci Linfedema Generalidades AnatomiaFeña Peña GonzalezPas encore d'évaluation
- Veterinary AnatomyDocument4 pagesVeterinary AnatomyDrRakesh Raki50% (2)
- ROLE OF STREPTOKINASE - OdpDocument7 pagesROLE OF STREPTOKINASE - OdpShumyle Mukhtar HussainPas encore d'évaluation
- Nclex Cardio QuestionsDocument4 pagesNclex Cardio QuestionsMichellePas encore d'évaluation
- Anatomy and Physiology SLEDocument27 pagesAnatomy and Physiology SLEMoti Pagador100% (4)
- Unit I (Hypertension) Part 1Document77 pagesUnit I (Hypertension) Part 1RUSSEL JAN ROJASPas encore d'évaluation
- The HeartDocument86 pagesThe HeartBlackHerbalsPas encore d'évaluation