Vous aimerez peut-être aussi
- Electrolyte Imbalance, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandElectrolyte Imbalance, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÉvaluation : 1 sur 5 étoiles1/5 (1)
- Fluids and Electrolytes FinalDocument50 pagesFluids and Electrolytes FinalOsego MokopotsaPas encore d'évaluation
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsD'EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsPas encore d'évaluation
- 3 Fluids and Electrolytes PPDocument112 pages3 Fluids and Electrolytes PPjcodoyPas encore d'évaluation
- Lec. 3 - Fluid and ElectrolyteDocument16 pagesLec. 3 - Fluid and Electrolyteمجيب سلطانPas encore d'évaluation
- Fluid Electrolyte and AcidBase BalanceDocument33 pagesFluid Electrolyte and AcidBase Balancemoncalshareen3Pas encore d'évaluation
- PCH 201 L 10.11.12 13Document25 pagesPCH 201 L 10.11.12 13KellyPas encore d'évaluation
- Lecture Notes 10, 11, 12 & 13: Water and Electrolytes HemostasisDocument25 pagesLecture Notes 10, 11, 12 & 13: Water and Electrolytes HemostasisKellyPas encore d'évaluation
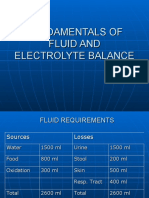
- Fundamentals of Fluid and Electrolyte BalanceDocument46 pagesFundamentals of Fluid and Electrolyte BalanceMelia Eka Rosita PharmacistPas encore d'évaluation
- Fluid and Electrolyte Balance and Fluid Therapy: Xiaoli Zhang The Third Affiliated Hospital of Zhengzhou UniversityDocument41 pagesFluid and Electrolyte Balance and Fluid Therapy: Xiaoli Zhang The Third Affiliated Hospital of Zhengzhou Universityapi-19916399Pas encore d'évaluation
- WaterDocument16 pagesWaterAUBREY LISAYENPas encore d'évaluation
- Kompartemen Cairan TubuhDocument27 pagesKompartemen Cairan Tubuhdalang leriPas encore d'évaluation
- Fluid & Electrolyte Balance: Part 4: Regulation & MaintenanceDocument40 pagesFluid & Electrolyte Balance: Part 4: Regulation & MaintenanceMy MusicPas encore d'évaluation
- Body Fluid 1Document55 pagesBody Fluid 1Anonymous z3afjyy1aPas encore d'évaluation
- S.No Table of Content Page NoDocument20 pagesS.No Table of Content Page NoTamilArasiPas encore d'évaluation
- Water and Electrolyte Balance: DR PreetiDocument116 pagesWater and Electrolyte Balance: DR PreetiSrishti GoenkaPas encore d'évaluation
- Fluid Blance SGDDocument11 pagesFluid Blance SGDChino Paolo SamsonPas encore d'évaluation
- Fluids Electrolytes - Acid-Base BalanceDocument11 pagesFluids Electrolytes - Acid-Base BalanceJhosita Flora Laroco100% (1)
- Fluid and Electrolyte Management of The Surgical Patient: DR TewodrosDocument45 pagesFluid and Electrolyte Management of The Surgical Patient: DR TewodrosBayisa GirmaPas encore d'évaluation
- Fluid and Electrolyte Imbalance PDFDocument21 pagesFluid and Electrolyte Imbalance PDFShafaq AlamPas encore d'évaluation
- Fluid, Electrolyte and Acid-Base BalanceDocument59 pagesFluid, Electrolyte and Acid-Base BalanceFlourence ZafranPas encore d'évaluation
- Fluids and Electrolytes Fluids and Electrolytes Acids, Bases, and Acids, Bases, and PH PH By: By: SMM SMM,, RN RN MD MD By: By: SMM SMM,, RN RN MD MDDocument50 pagesFluids and Electrolytes Fluids and Electrolytes Acids, Bases, and Acids, Bases, and PH PH By: By: SMM SMM,, RN RN MD MD By: By: SMM SMM,, RN RN MD MDRose AlmanzorPas encore d'évaluation
- Water and Electrolyte ImbalanceDocument17 pagesWater and Electrolyte Imbalancemhairat6043100% (1)
- 2040fe Part2Document15 pages2040fe Part2clubsingr28Pas encore d'évaluation
- Nursing Care Plan of Client With Fluid and Electrolyte ImbalanceDocument28 pagesNursing Care Plan of Client With Fluid and Electrolyte ImbalanceCj Aguilar50% (2)
- Fundamentals of Fluid and Electrolyte Balance Parenteral SolutionsDocument55 pagesFundamentals of Fluid and Electrolyte Balance Parenteral SolutionsTri RachmadijantoPas encore d'évaluation
- normal Exchange of Fluids &electrolytes 2. Classification of Body Fluid ChangesDocument31 pagesnormal Exchange of Fluids &electrolytes 2. Classification of Body Fluid ChangesRajarshi KumarPas encore d'évaluation
- F and e Imb .... Edu ..Document20 pagesF and e Imb .... Edu ..esakkiammalPas encore d'évaluation
- Chapter 27: Fluid and Electrolyte BalanceDocument26 pagesChapter 27: Fluid and Electrolyte BalanceMarwan M.Pas encore d'évaluation
- Fluid and Electrolyte Management-1Document40 pagesFluid and Electrolyte Management-1hossein boloorianPas encore d'évaluation
- Biochemistry-Module 10 (Electrolytes)Document11 pagesBiochemistry-Module 10 (Electrolytes)Rommel BaraquielPas encore d'évaluation
- Case Study HyperkalemiaDocument10 pagesCase Study HyperkalemiaJamaica Cerrero100% (1)
- Physiology 1 Fluid ElectrolyteDocument38 pagesPhysiology 1 Fluid ElectrolyteHaziq KamardinPas encore d'évaluation
- Class Presentated by Anima Layek: Fluid and Electrolyte ImbalanceDocument39 pagesClass Presentated by Anima Layek: Fluid and Electrolyte ImbalanceTumpa ShitPas encore d'évaluation
- AC. Nutrition - Water and ElectrolytesDocument81 pagesAC. Nutrition - Water and ElectrolytesAnuchithra Radhakrishnan100% (1)
- FLuid & Elect & Acid Base & Surg. Nutr.Document24 pagesFLuid & Elect & Acid Base & Surg. Nutr.anon_761270640Pas encore d'évaluation
- Fluids and ElectrolytesDocument48 pagesFluids and ElectrolytesChernobyle Tolentino BattadPas encore d'évaluation
- Electrolytes: Electrolytes Also Regulate Many Vital Processes in Our BodyDocument4 pagesElectrolytes: Electrolytes Also Regulate Many Vital Processes in Our BodyMichelle ViduyaPas encore d'évaluation
- Final Water ElectrolytesDocument97 pagesFinal Water ElectrolytesMonika shankarPas encore d'évaluation
- Body Fluids and ElectrolytesDocument42 pagesBody Fluids and ElectrolytesQusaiBadr100% (1)
- 6.0 ElectrolytesDocument4 pages6.0 ElectrolytesHry WkPas encore d'évaluation
- Fluid and Electrolyte BalanceDocument87 pagesFluid and Electrolyte Balancerajashree kokatanurPas encore d'évaluation
- Meeting The Needs of The PatientDocument33 pagesMeeting The Needs of The PatientMuneeswaran SmpPas encore d'évaluation
- Basic Renal NotesDocument4 pagesBasic Renal Notesyannie.s.liPas encore d'évaluation
- Potassium Metabolism MainDocument59 pagesPotassium Metabolism MainPrincewill SeiyefaPas encore d'évaluation
- 3 Fluid and ElectrolyteDocument7 pages3 Fluid and ElectrolyteStephen HDPas encore d'évaluation
- Major IntracelularDocument67 pagesMajor Intracelularfarooq shah shabbirPas encore d'évaluation
- Fluid and Electrolyte General Surgery Review Course.Document97 pagesFluid and Electrolyte General Surgery Review Course.Kamil HannaPas encore d'évaluation
- Water and Sodium 2024 PDFDocument61 pagesWater and Sodium 2024 PDFMpho MosehlaPas encore d'évaluation
- New Fluid and Electrolytes Therapy Toyinoriginali2againDocument55 pagesNew Fluid and Electrolytes Therapy Toyinoriginali2againt.baby100% (1)
- Fluids: ElectrolytesDocument56 pagesFluids: ElectrolytesZee Zang100% (1)
- Fluids and ElectrolytesDocument49 pagesFluids and ElectrolytesMoon KillerPas encore d'évaluation
- F and 1Document51 pagesF and 1api-19641337Pas encore d'évaluation
- Mabes Fluid and ElectrolytesDocument9 pagesMabes Fluid and ElectrolytesMabesPas encore d'évaluation
- 19 Fluid and Electrolyte Imbalance and Nutritional ProblemDocument40 pages19 Fluid and Electrolyte Imbalance and Nutritional ProblemPaul EbenezerPas encore d'évaluation
- Fluids & Electrolytes: April Love Rivera-Oja, RN-MANDocument56 pagesFluids & Electrolytes: April Love Rivera-Oja, RN-MANAdelin MeroPas encore d'évaluation
- Fluid, Electrolyte, and Acid-Base Balance: Prepared by Janice Meeking, Mount Royal CollegeDocument96 pagesFluid, Electrolyte, and Acid-Base Balance: Prepared by Janice Meeking, Mount Royal CollegeRajesh KumarPas encore d'évaluation
- Intravenous Fluids: Composition & UsesDocument41 pagesIntravenous Fluids: Composition & UsesFathima BanuzPas encore d'évaluation
- Clinical Biochemistry - ElektifDocument84 pagesClinical Biochemistry - ElektifAni RianiPas encore d'évaluation
- Fluid, Electrolyte and Acid-Base BalanceDocument42 pagesFluid, Electrolyte and Acid-Base BalanceMiss Vina100% (1)
- Community Diagnosis Tramo Uno, San Dionisio, Paranaque CityDocument85 pagesCommunity Diagnosis Tramo Uno, San Dionisio, Paranaque CityanreilegardePas encore d'évaluation
- Micu MedsDocument3 pagesMicu MedsanreilegardePas encore d'évaluation
- PRC Midwifery FormsDocument4 pagesPRC Midwifery Formsjhimeady92% (12)
- Planning - Nursing Management FunctionDocument27 pagesPlanning - Nursing Management Functionanreilegarde100% (17)
- Physical Assessment FormatDocument4 pagesPhysical Assessment Formatanreilegarde67% (3)
- Resume' of AnreiDocument3 pagesResume' of AnreianreilegardePas encore d'évaluation
- Nursing Care Plan FormatDocument2 pagesNursing Care Plan FormatanreilegardePas encore d'évaluation
- Directing Nursing ManagementDocument26 pagesDirecting Nursing Managementanreilegarde86% (7)
- Nepal Bhutan Maldives ComparisonsDocument2 pagesNepal Bhutan Maldives ComparisonsanreilegardePas encore d'évaluation
- Controlling - Nursing ManagementDocument43 pagesControlling - Nursing Managementanreilegarde94% (18)
- Staffing Nursing ManagementDocument55 pagesStaffing Nursing Managementanreilegarde90% (20)
- Organizing - Nursing ManagementDocument104 pagesOrganizing - Nursing Managementanreilegarde100% (19)
- Nursing Leadership and Its TheoriesDocument71 pagesNursing Leadership and Its Theoriesanreilegarde100% (1)
- Nursing Management IntroductionDocument42 pagesNursing Management Introductionanreilegarde100% (5)
- Osteogenesis ImperfectaDocument8 pagesOsteogenesis ImperfectaDokter ZukiePas encore d'évaluation
- Physical Assessment of School Age Children - SCHOOL NURSINGDocument3 pagesPhysical Assessment of School Age Children - SCHOOL NURSINGanreilegarde100% (8)
- SuicideDocument10 pagesSuicideanreilegardePas encore d'évaluation
- Sjdefi PRC Forms SignatoriesDocument1 pageSjdefi PRC Forms SignatoriesanreilegardePas encore d'évaluation
- Pyrazinamide Drug StudyDocument1 pagePyrazinamide Drug Studyanreilegarde100% (2)
- All About Resume and Curriculum VitaeDocument8 pagesAll About Resume and Curriculum VitaeanreilegardePas encore d'évaluation
- MR - Molina's P.A and Nursing HistoryDocument4 pagesMR - Molina's P.A and Nursing HistoryanreilegardePas encore d'évaluation
- Planning - Nursing Management FunctionDocument27 pagesPlanning - Nursing Management Functionanreilegarde100% (17)
- Eating Disorders - LectureDocument53 pagesEating Disorders - LectureanreilegardePas encore d'évaluation
- Malaria: Causative OrganismsDocument5 pagesMalaria: Causative OrganismsanreilegardePas encore d'évaluation
- Blood Disorders - LeukemiaDocument24 pagesBlood Disorders - LeukemiaanreilegardePas encore d'évaluation
- Psychiatric Nursing: Mood DisordersDocument31 pagesPsychiatric Nursing: Mood DisordersanreilegardePas encore d'évaluation
- Upper Respiratory DiseasesDocument3 pagesUpper Respiratory DiseasesanreilegardePas encore d'évaluation
- General Management For Potts DiseaseDocument2 pagesGeneral Management For Potts Diseaseanreilegarde100% (1)
- Review of Orthopedic NursingDocument19 pagesReview of Orthopedic Nursinganreilegarde100% (1)
- Bacterial Meningitis Signs and SymptomsDocument2 pagesBacterial Meningitis Signs and SymptomsanreilegardePas encore d'évaluation
- Basics of An Model United Competition, Aippm, All India Political Parties' Meet, Mun Hrishkesh JaiswalDocument7 pagesBasics of An Model United Competition, Aippm, All India Political Parties' Meet, Mun Hrishkesh JaiswalHRISHIKESH PRAKASH JAISWAL100% (1)
- Phylogenetic Tree: GlossaryDocument7 pagesPhylogenetic Tree: GlossarySab ka bada FanPas encore d'évaluation
- School Games Calendar Part-1Document5 pagesSchool Games Calendar Part-1Ranadhir Singh100% (2)
- CS 124/LINGUIST 180 From Languages To Information: Conversational AgentsDocument58 pagesCS 124/LINGUIST 180 From Languages To Information: Conversational AgentsamanPas encore d'évaluation
- TIMELINE - Philippines of Rizal's TimesDocument46 pagesTIMELINE - Philippines of Rizal's TimesAntonio Delgado100% (1)
- What Is An Ethical Dilemma?: Decision-Making ProcessDocument7 pagesWhat Is An Ethical Dilemma?: Decision-Making ProcessGauravsPas encore d'évaluation
- Item AnalysisDocument7 pagesItem AnalysisJeff LestinoPas encore d'évaluation
- Curriculum Vitae: Personal InformationDocument2 pagesCurriculum Vitae: Personal InformationtyasPas encore d'évaluation
- ICTSAS601 Student Assessment Tasks 2020Document30 pagesICTSAS601 Student Assessment Tasks 2020Lok SewaPas encore d'évaluation
- Sabbir 47MDocument25 pagesSabbir 47MMd.sabbir Hossen875Pas encore d'évaluation
- Jurnal Perdata K 1Document3 pagesJurnal Perdata K 1Edi nur HandokoPas encore d'évaluation
- 1-Gaikindo Category Data Jandec2020Document2 pages1-Gaikindo Category Data Jandec2020Tanjung YanugrohoPas encore d'évaluation
- Ikramul (Electrical)Document3 pagesIkramul (Electrical)Ikramu HaquePas encore d'évaluation
- Post Cold WarDocument70 pagesPost Cold WarZainab WaqarPas encore d'évaluation
- Foucault, M.-Experience-Book (Trombadori Interview)Document11 pagesFoucault, M.-Experience-Book (Trombadori Interview)YashinPas encore d'évaluation
- 6401 1 NewDocument18 pages6401 1 NewbeeshortPas encore d'évaluation
- Assignment 2 Malaysian StudiesDocument4 pagesAssignment 2 Malaysian StudiesPenny PunPas encore d'évaluation
- Meditation For AddictionDocument2 pagesMeditation For AddictionharryPas encore d'évaluation
- Company Profile ESB Update May 2021 Ver 1Document9 pagesCompany Profile ESB Update May 2021 Ver 1Nakaturi CoffeePas encore d'évaluation
- Iii. The Impact of Information Technology: Successful Communication - Key Points To RememberDocument7 pagesIii. The Impact of Information Technology: Successful Communication - Key Points To Remembermariami bubuPas encore d'évaluation
- Marriot CaseDocument15 pagesMarriot CaseArsh00100% (7)
- PUERPERAL SEPSIS CoverDocument9 pagesPUERPERAL SEPSIS CoverKerpersky LogPas encore d'évaluation
- Hellwalker: "What Terrors Do You Think I Have Not Already Seen?"Document2 pagesHellwalker: "What Terrors Do You Think I Have Not Already Seen?"mpotatoPas encore d'évaluation
- Lifeline® Specialty: Fire Resistant QFCI Cable: Fire Resistant, Flame Retardant Halogen-Free Loose Tube - QFCI/O/RM-JMDocument2 pagesLifeline® Specialty: Fire Resistant QFCI Cable: Fire Resistant, Flame Retardant Halogen-Free Loose Tube - QFCI/O/RM-JMkevinwz1989Pas encore d'évaluation
- National Rural Employment Guarantee Act, 2005Document17 pagesNational Rural Employment Guarantee Act, 2005praharshithaPas encore d'évaluation
- FAMILYDocument3 pagesFAMILYJenecel ZanoriaPas encore d'évaluation
- LBST 2102 Final EssayDocument9 pagesLBST 2102 Final Essayapi-318174977Pas encore d'évaluation
- Grope Assignment 1Document5 pagesGrope Assignment 1SELAM APas encore d'évaluation
- Management of Graves Disease 2015 JAMA ADocument11 pagesManagement of Graves Disease 2015 JAMA AMade ChandraPas encore d'évaluation
- Rid and Clean Safety DataDocument1 pageRid and Clean Safety DataElizabeth GracePas encore d'évaluation