Vous aimerez peut-être aussi
- Adjustment and Impulse Control DisordersDocument19 pagesAdjustment and Impulse Control DisordersArchana50% (4)
- Nutritional AnemiaDocument53 pagesNutritional AnemiaANUREET KAURPas encore d'évaluation
- Achieving Newborn Care CompetencyDocument2 pagesAchieving Newborn Care CompetencyShekaina BartidoPas encore d'évaluation
- Vital Rates and RatiosDocument2 pagesVital Rates and RatiossrhmdPas encore d'évaluation
- A Strategic Management PaperDocument7 pagesA Strategic Management PaperKarll Brendon SalubrePas encore d'évaluation
- German BasicDocument60 pagesGerman BasicchahirPas encore d'évaluation
- Normal Laboratory Values - Patient Test Reference RangesDocument10 pagesNormal Laboratory Values - Patient Test Reference RangesGita Elisa Berlina GintingPas encore d'évaluation
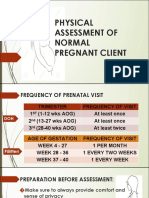
- Physical Assessment of a Pregnant ClientDocument25 pagesPhysical Assessment of a Pregnant ClientDe Leon, Austine Sydney D.Pas encore d'évaluation
- A Momentum Trading StrategyDocument11 pagesA Momentum Trading StrategyObinna Obiefule67% (3)
- A Momentum Trading StrategyDocument11 pagesA Momentum Trading StrategyObinna Obiefule67% (3)
- Medical Disorder During PregnancyDocument310 pagesMedical Disorder During PregnancyRitbano AhmedPas encore d'évaluation
- Approach To Neonatal HyperbilirubinemiaDocument34 pagesApproach To Neonatal HyperbilirubinemiaNilesh HatzadePas encore d'évaluation
- Caribbean Studies - Lesson 8 - Concept and Indicator of Development PDFDocument37 pagesCaribbean Studies - Lesson 8 - Concept and Indicator of Development PDFDarrion BrucePas encore d'évaluation
- Withdrawal (Coitus Interruptus)Document9 pagesWithdrawal (Coitus Interruptus)Mochammad Adam EldiPas encore d'évaluation
- Elderly PrimigravidaDocument7 pagesElderly PrimigravidaAnonymous mvNUtwidPas encore d'évaluation
- Icu Adult and PaedsDocument2 pagesIcu Adult and PaedsPrashin RocharamPas encore d'évaluation
- Updates/Refresher For BHWS' Rules and Functions:: Inayangan Health Center Calinan DistrictDocument26 pagesUpdates/Refresher For BHWS' Rules and Functions:: Inayangan Health Center Calinan Districtbryan john barbosaPas encore d'évaluation
- PATIENT 1 Nursing Assessment FormDocument5 pagesPATIENT 1 Nursing Assessment FormndembolovePas encore d'évaluation
- PedsCases Script AW FinalDocument13 pagesPedsCases Script AW FinalShubhrima KhanPas encore d'évaluation
- Kandungan Buku Perinatal Care Manual 4th Edition - 1jun2022Document14 pagesKandungan Buku Perinatal Care Manual 4th Edition - 1jun2022Zarif SyafiqPas encore d'évaluation
- National Dengue Prevention ProgramDocument26 pagesNational Dengue Prevention ProgramFranz Anthony Quirit GoPas encore d'évaluation
- Openstack Deployment Ops Guide PDFDocument197 pagesOpenstack Deployment Ops Guide PDFBinank PatelPas encore d'évaluation
- NLEP Annual Report - 2016-17 - RevDocument23 pagesNLEP Annual Report - 2016-17 - RevMOORTHY.KEPas encore d'évaluation
- Public Health CommunityDocument10 pagesPublic Health CommunityGummy BearsPas encore d'évaluation
- Study On Menstruation and Hygiene Practices Among Adolescent Girls in Urban CommunityDocument5 pagesStudy On Menstruation and Hygiene Practices Among Adolescent Girls in Urban CommunitydeepaPas encore d'évaluation
- Pediatric DKA: Section I: Scenario DemographicsDocument8 pagesPediatric DKA: Section I: Scenario DemographicsSherein ShalabyPas encore d'évaluation
- Sec D - Intervention of Common Signs & SymptomsDocument30 pagesSec D - Intervention of Common Signs & SymptomsCheryl OrtizPas encore d'évaluation
- Understanding Post-term Pregnancy ManagementDocument16 pagesUnderstanding Post-term Pregnancy Managementahmed shorsh100% (1)
- Menstruation and Menstrual Hygiene Management in Selected KwaZulu-Natal SchoolsDocument52 pagesMenstruation and Menstrual Hygiene Management in Selected KwaZulu-Natal SchoolsOxfamPas encore d'évaluation
- 4.hyperemesis & Amniotic Fluid DisorderDocument53 pages4.hyperemesis & Amniotic Fluid DisorderjosephPas encore d'évaluation
- 10 PrematurityDocument20 pages10 PrematurityAyman Elsir100% (1)
- Vital SignsDocument38 pagesVital SignsSanjna Kumari (SNSR Senior Tutor/Lecturer)100% (1)
- Q Oral Glucose Tolerance TestDocument4 pagesQ Oral Glucose Tolerance TestNur Amirah FarhanahPas encore d'évaluation
- Protein Calorie MalnutritionDocument97 pagesProtein Calorie Malnutritionnshaikh56Pas encore d'évaluation
- Menstrual Hygiene - Research MethodologyDocument7 pagesMenstrual Hygiene - Research MethodologyAnjali PandeyPas encore d'évaluation
- N102 CONCEPT PAPER-breastfeeding PracticesDocument16 pagesN102 CONCEPT PAPER-breastfeeding PracticesKay Star TamayoPas encore d'évaluation
- Neonatal SepsisDocument51 pagesNeonatal SepsisAngelo Del VentoPas encore d'évaluation
- CHW Roles and TasksDocument30 pagesCHW Roles and TasksdanielPas encore d'évaluation
- Health Assessment 2Document9 pagesHealth Assessment 2Mandira NagPas encore d'évaluation
- Pharmacology Monitoring Medication LevelsDocument8 pagesPharmacology Monitoring Medication LevelsThierd Cañete III100% (1)
- Iron Dextran (Cosmofer) - ChartDocument1 pageIron Dextran (Cosmofer) - ChartDerrick Ezra NgPas encore d'évaluation
- Acute Renal Failure & Chronic Renal FailureDocument38 pagesAcute Renal Failure & Chronic Renal FailureArti GondPas encore d'évaluation
- Normalpuerperium 200523093433Document99 pagesNormalpuerperium 200523093433STANN KAZIPETPas encore d'évaluation
- Oral Contraceptive PillDocument21 pagesOral Contraceptive Pillherlanboga100% (1)
- Menstrual HygieneDocument8 pagesMenstrual HygieneManvendra Pratap SinghPas encore d'évaluation
- Guillain-Barré Syndrome in a 5-Year-Old GirlDocument33 pagesGuillain-Barré Syndrome in a 5-Year-Old GirlYoel RayPas encore d'évaluation
- COMMUNITY HEALTH NURSING (PRELIMSDocument36 pagesCOMMUNITY HEALTH NURSING (PRELIMSPCIs DR RotationPas encore d'évaluation
- Nursing Student Objectives and Patient Diagnostic ReportsDocument5 pagesNursing Student Objectives and Patient Diagnostic ReportsRae Marie AquinoPas encore d'évaluation
- Newborn Eye Prophylaxis and Vaccines ExplainedDocument14 pagesNewborn Eye Prophylaxis and Vaccines ExplainedJoiz Rivera100% (2)
- A Healthy Nation Is A Wealthy Nation (Philosophy)Document3 pagesA Healthy Nation Is A Wealthy Nation (Philosophy)tickler007100% (3)
- GEN GallBladderInstrumentsADocument10 pagesGEN GallBladderInstrumentsANeo Rodriguez AlvaradoPas encore d'évaluation
- Under Nutrition and Its Associated Factors Among Adolescent Girls in Rural Community of Aseko District, Eastern Arsi Zone, Oromia Region, Eastern Ethiopia, 2017Document10 pagesUnder Nutrition and Its Associated Factors Among Adolescent Girls in Rural Community of Aseko District, Eastern Arsi Zone, Oromia Region, Eastern Ethiopia, 2017Anonymous SMEU6r2Pas encore d'évaluation
- Supraventricular TachycardiaDocument22 pagesSupraventricular TachycardiaFaza KahfiPas encore d'évaluation
- Labor Curve & Partograph GuideDocument50 pagesLabor Curve & Partograph GuideJhervy VillanuevaPas encore d'évaluation
- St. Joseph Mercy Ann Arbor Sepsis Screening ToolDocument2 pagesSt. Joseph Mercy Ann Arbor Sepsis Screening ToolArnelli HutagalungPas encore d'évaluation
- Community Health Profile of Barangay DimagibaDocument184 pagesCommunity Health Profile of Barangay Dimagibastephanie valerioPas encore d'évaluation
- Maternal Resuscitation DrillDocument23 pagesMaternal Resuscitation Drillapi-219741636100% (2)
- Acute Renal Failure Pathophysiology, Stages, Complications & ManagementDocument18 pagesAcute Renal Failure Pathophysiology, Stages, Complications & ManagementSteven Paul DaclesPas encore d'évaluation
- BreastfeedingDocument111 pagesBreastfeedingabdur rahman zulkifliPas encore d'évaluation
- NITI Aayog - WikipediaDocument22 pagesNITI Aayog - WikipediaKirti RajputPas encore d'évaluation
- Ati Codes Cont'Document1 pageAti Codes Cont'm1k0ePas encore d'évaluation
- A-Nutritional Deficiency FN IIIDocument45 pagesA-Nutritional Deficiency FN IIIashamartinaPas encore d'évaluation
- Reduce LBW Incidence in IndiaDocument24 pagesReduce LBW Incidence in IndiaNabanita Tania DePas encore d'évaluation
- Nutrition Needs During PregnancyDocument25 pagesNutrition Needs During PregnancyTony KhattarPas encore d'évaluation
- Kidney Disease and PregnancyDocument11 pagesKidney Disease and PregnancyAndreaPas encore d'évaluation
- AnemiaMukt Bharat I-NIPIDocument23 pagesAnemiaMukt Bharat I-NIPIMukunda MurariPas encore d'évaluation
- Teen Pregnancy PreventionDocument9 pagesTeen Pregnancy PreventionJoshua Emmanuel LedesmaPas encore d'évaluation
- Iprantitb AdrDocument53 pagesIprantitb AdrHafiiz ShafiiPas encore d'évaluation
- 24hr Urine ProteinDocument1 page24hr Urine ProteinHafiiz ShafiiPas encore d'évaluation
- Physiotherapy Vs OTDocument1 pagePhysiotherapy Vs OTHafiiz ShafiiPas encore d'évaluation
- Anxiety DisorderDocument56 pagesAnxiety DisorderHafiiz ShafiiPas encore d'évaluation
- Untitled DocumentDocument2 pagesUntitled DocumentChristopher BellardPas encore d'évaluation
- Plant Processes: Lesson 3Document3 pagesPlant Processes: Lesson 3Kayla Ta’jaePas encore d'évaluation
- Atlanta Pipes and FittingsDocument2 pagesAtlanta Pipes and Fittingsotadoyreychie31Pas encore d'évaluation
- JNTUA Mechanical Engineering (R09) Syllabus BookDocument147 pagesJNTUA Mechanical Engineering (R09) Syllabus Bookslv_prasaad0% (1)
- Manage a micro business with BSB30315Document3 pagesManage a micro business with BSB30315Theo A W JacksonPas encore d'évaluation
- ExportDocument18 pagesExportDolon MukherjeePas encore d'évaluation
- Nodelman 1992Document8 pagesNodelman 1992Ana Luiza RochaPas encore d'évaluation
- Oposa vs. Factoran 224 Scra 792Document28 pagesOposa vs. Factoran 224 Scra 792albemartPas encore d'évaluation
- Bioav 3Document264 pagesBioav 3Sabiruddin Mirza DipuPas encore d'évaluation
- VIACRYL VSC 6250w/65MP: Technical DatasheetDocument2 pagesVIACRYL VSC 6250w/65MP: Technical DatasheetPratik MehtaPas encore d'évaluation
- Datasheet AD549Document14 pagesDatasheet AD549Trần Hồng VănPas encore d'évaluation
- DX DiagDocument42 pagesDX DiagVinvin PatrimonioPas encore d'évaluation
- Macbeth Introduction0Document40 pagesMacbeth Introduction0MohammedelaminePas encore d'évaluation
- Good Evil EssayDocument2 pagesGood Evil EssayuniquebythemillionsPas encore d'évaluation
- Health Benefits of Kidney BeansDocument17 pagesHealth Benefits of Kidney BeansShyneAneeshPas encore d'évaluation
- CANAVAN' and VESCOVI - 2004 - CMJ X SJ Evaluation of Power Prediction Equations Peak Vertical Jumping Power in WomenDocument6 pagesCANAVAN' and VESCOVI - 2004 - CMJ X SJ Evaluation of Power Prediction Equations Peak Vertical Jumping Power in WomenIsmenia HelenaPas encore d'évaluation
- Atomic Structure - One Shot by Sakshi Mam #BounceBackDocument231 pagesAtomic Structure - One Shot by Sakshi Mam #BounceBackchansiray7870Pas encore d'évaluation
- Nec TutorialDocument5 pagesNec TutorialbheemasenaPas encore d'évaluation
- Working Capital Management (2015)Document62 pagesWorking Capital Management (2015)AJPas encore d'évaluation
- Sankalp Sanjeevani NEET: PhysicsDocument11 pagesSankalp Sanjeevani NEET: PhysicsKey RavenPas encore d'évaluation
- Impacts of DecarbonizationDocument2 pagesImpacts of DecarbonizationCM SoongPas encore d'évaluation
- MarasiNews Issue 12Document47 pagesMarasiNews Issue 12Sunil Kumar P GPas encore d'évaluation
- 1st ClassDocument18 pages1st Classchitl.23bi14075Pas encore d'évaluation
- Srimanta Shankardev: Early LifeDocument3 pagesSrimanta Shankardev: Early LifeAnusuya BaruahPas encore d'évaluation
- Specification: F.V/Tim e 3min 5min 8min 10MIN 15MIN 20MIN 30MIN 60MIN 90MIN 1.60V 1.67V 1.70V 1.75V 1.80V 1.85VDocument2 pagesSpecification: F.V/Tim e 3min 5min 8min 10MIN 15MIN 20MIN 30MIN 60MIN 90MIN 1.60V 1.67V 1.70V 1.75V 1.80V 1.85VJavierPas encore d'évaluation