Vous aimerez peut-être aussi
- 10,000 ReasonsDocument9 pages10,000 ReasonsStephanie BragatPas encore d'évaluation
- Pharma Compre SamplexDocument19 pagesPharma Compre SamplexStephanie BragatPas encore d'évaluation
- Semen AnalysisDocument2 pagesSemen AnalysisStephanie BragatPas encore d'évaluation
- Epi AssignmentDocument2 pagesEpi AssignmentStephanie BragatPas encore d'évaluation
- Stress Coping Style 2Document20 pagesStress Coping Style 2Stephanie Bragat0% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- PulpotecDocument2 pagesPulpotecFeras Al-ZbounPas encore d'évaluation
- Surgical Wound ClassificationDocument1 pageSurgical Wound Classificationgeclear323Pas encore d'évaluation
- Trivia About San Lazaro HospitalDocument2 pagesTrivia About San Lazaro Hospitalsaiyuki00450% (2)
- NCP 2 QiDocument3 pagesNCP 2 QiKarlo Tuazon SedigoPas encore d'évaluation
- Chapter 4 Drug StudyDocument9 pagesChapter 4 Drug StudyRegee Rose LacsonPas encore d'évaluation
- The Pathogenesis of Optic Neuritis Caused by Angiostrongylus Cantonensis in BALB/c MiceDocument12 pagesThe Pathogenesis of Optic Neuritis Caused by Angiostrongylus Cantonensis in BALB/c Miceracut_khansatraPas encore d'évaluation
- Partial Genome Characterization of Novel ParapoxviDocument4 pagesPartial Genome Characterization of Novel Parapoxviali zohaibPas encore d'évaluation
- Vantocil IB Antimicrobial-Antiviral ActivityDocument5 pagesVantocil IB Antimicrobial-Antiviral ActivityMinh LêPas encore d'évaluation
- Interesting Facts About Yailin La Mas ViralijomiDocument2 pagesInteresting Facts About Yailin La Mas Viralijomiscentbeast8Pas encore d'évaluation
- PDS - Metazolone-FM - Ver 2.0Document1 pagePDS - Metazolone-FM - Ver 2.0Rama KrishnanPas encore d'évaluation
- Internal MedicineDocument277 pagesInternal MedicineAhmad Abu ArkoubPas encore d'évaluation
- CPH Final ReviewersDocument10 pagesCPH Final ReviewersANDRIANNE FAGUTAOPas encore d'évaluation
- Engish 1st Language MCQ's Question BankDocument77 pagesEngish 1st Language MCQ's Question BankShivalingappa Sampaganvi67% (3)
- T.Y. B.Sc. Microbiology (June-2008)Document17 pagesT.Y. B.Sc. Microbiology (June-2008)Mihir MistryPas encore d'évaluation
- Fowl PoxDocument17 pagesFowl PoxUsman KhalidPas encore d'évaluation
- Doh Infection Prevention & Control Training Manual: Volume II For Health Facility AdministratorsDocument119 pagesDoh Infection Prevention & Control Training Manual: Volume II For Health Facility AdministratorsAlex SanchezPas encore d'évaluation
- TonsilofaringitisDocument1 pageTonsilofaringitisFadhli Rajif TangkePas encore d'évaluation
- Bubonic Plague Research Paper OutlineDocument4 pagesBubonic Plague Research Paper Outlinegvyns594100% (3)
- Abernathy 1Document2 pagesAbernathy 1api-316558435Pas encore d'évaluation
- Sore Throat, Hoarseness and Otitis MediaDocument19 pagesSore Throat, Hoarseness and Otitis MediaainaPas encore d'évaluation
- HES 007 2nd Periodical Exam TG Day 17Document3 pagesHES 007 2nd Periodical Exam TG Day 17AlbieRhioneilLatonioMacayanPas encore d'évaluation
- 05-S-2019 Dengue Ordinance of Barangay San CarlosDocument6 pages05-S-2019 Dengue Ordinance of Barangay San CarlosRonel Rosal MalunesPas encore d'évaluation
- FYP MSC Biotch ReportDocument66 pagesFYP MSC Biotch ReportGaurav ChauhanPas encore d'évaluation
- Hooper David - The Colloidal Silver Hand BookDocument23 pagesHooper David - The Colloidal Silver Hand BookStarla ShermanPas encore d'évaluation
- Assignment On Designing A Communication Campaign For Mexico About HIVDocument11 pagesAssignment On Designing A Communication Campaign For Mexico About HIVxhuvo50% (2)
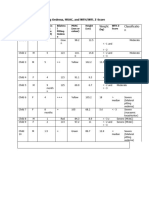
- PART C. Bilateral Pitting Oedema, MUAC, and WFH/WFL Z-Score: Weight Classificatio NDocument12 pagesPART C. Bilateral Pitting Oedema, MUAC, and WFH/WFL Z-Score: Weight Classificatio NFeiruzPas encore d'évaluation
- IARC Sci Pub 163 - Chapter 10Document14 pagesIARC Sci Pub 163 - Chapter 10ashin411Pas encore d'évaluation
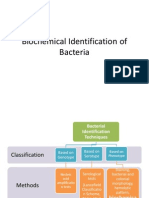
- Biochemical Identification of BacteriaDocument72 pagesBiochemical Identification of BacteriaMaria Jhoyce MagpantayPas encore d'évaluation
- 29725Document10 pages29725zzzzPas encore d'évaluation
- Module 2 - PLANNING (Davao)Document20 pagesModule 2 - PLANNING (Davao)Anne Abejuela ObialPas encore d'évaluation