Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- My FamilyDocument4 pagesMy FamilyGodfather292Pas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Food RecipeDocument2 pagesFood RecipeGodfather292Pas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- AlcoholDocument2 pagesAlcoholGodfather292Pas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Inspire Papdi Modul CD 1Document125 pagesInspire Papdi Modul CD 1Ika BelindaPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Food Safety Issues in Asia, SEAFAST PDFDocument35 pagesFood Safety Issues in Asia, SEAFAST PDFRezaAbdifiPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Assignment - Define DrugDocument10 pagesAssignment - Define DrugDaiyne C. CarbonPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Bells Palsy FPUK Web PDFDocument11 pagesBells Palsy FPUK Web PDFRadhaKrishnanPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Foundation of Guidance 1Document16 pagesFoundation of Guidance 1leo sentelicesPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Obsessional Neurosis and InhibitionDocument17 pagesObsessional Neurosis and InhibitionVladan K. StojanovićPas encore d'évaluation
- Tai Chi For Health PurposesDocument7 pagesTai Chi For Health PurposesClaire18Pas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- MPS Therapy Flyer April 10 2018Document8 pagesMPS Therapy Flyer April 10 2018Neptune ShellPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Kasus 1 RKG 5 Euginia YosephineDocument5 pagesKasus 1 RKG 5 Euginia YosephineEuginia YosephinePas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- 112公私立第三次 重點單字片語整理 (PARTII)Document10 pages112公私立第三次 重點單字片語整理 (PARTII)黃紘志Pas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- 11 Antihypertensive AgentsDocument43 pages11 Antihypertensive AgentsAnonymous pmMHrWHdPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Harry Stack SullivanDocument2 pagesHarry Stack Sullivanlaine_mbz09100% (1)
- CH 35 Dental Handpieces and Accessories3641Document32 pagesCH 35 Dental Handpieces and Accessories3641Suvasish Suvasish50% (2)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- PADI MarineInjuries Specialty OutlineDocument1 pagePADI MarineInjuries Specialty OutlineFreddys DivePas encore d'évaluation
- Prostate Cancer Basic MechanismsDocument450 pagesProstate Cancer Basic MechanismsAhlan SyahrezaPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- HemerroidDocument24 pagesHemerroidVina WinePas encore d'évaluation
- Baclofen (Drug Study)Document2 pagesBaclofen (Drug Study)Franz.thenurse6888100% (1)
- Gene Therapy: Science, Technology and SocietyDocument18 pagesGene Therapy: Science, Technology and SocietyTricia AcordaPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Neurogenesis: The Amygdala and The HippocampusDocument3 pagesNeurogenesis: The Amygdala and The HippocampusAnonymous j3gtTw100% (1)
- Freud Life and WorksDocument11 pagesFreud Life and WorksAnomarPas encore d'évaluation
- Counselling PsychologyDocument63 pagesCounselling PsychologyEddy MwachenjePas encore d'évaluation
- 2.5 Digoxin ToxicityDocument8 pages2.5 Digoxin ToxicityWaqar WikiPas encore d'évaluation
- Low Dose KetamineDocument13 pagesLow Dose KetamineAndrias OzPas encore d'évaluation
- AnticholinergicsDocument33 pagesAnticholinergicspramod bhaleraoPas encore d'évaluation
- Updated at ResumeDocument3 pagesUpdated at Resumeapi-356396463Pas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Unit - I: Introduction To Pediatric NursingDocument45 pagesUnit - I: Introduction To Pediatric Nursingbereket gashu100% (2)
- Benign Prostate HyperplasiaDocument6 pagesBenign Prostate HyperplasiaFreddy PanjaitanPas encore d'évaluation
- Blood DonationDocument76 pagesBlood Donationlanie_bluegirl100% (1)
- 50 State Survey - Scope - 07.2015Document85 pages50 State Survey - Scope - 07.2015Anonymous kdBDppigEPas encore d'évaluation
- Direct Decision TherapyDocument9 pagesDirect Decision TherapyzarrarPas encore d'évaluation
- Cri 188 FinalsDocument12 pagesCri 188 FinalsKaren Angel AbaoPas encore d'évaluation
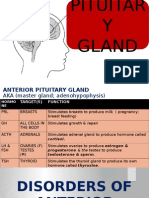
- Disorders of Pituitary GlandDocument34 pagesDisorders of Pituitary GlandninaaltheaPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)