Vous aimerez peut-être aussi
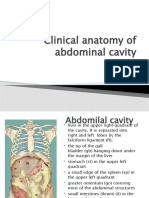
- Clinical Anatomy of Abdominal CavityDocument88 pagesClinical Anatomy of Abdominal CavityFahim NadvyPas encore d'évaluation
- Pediatric Surgery PresentationDocument191 pagesPediatric Surgery PresentationdanoonotPas encore d'évaluation
- Topographic Anatomy and Operative Surgery of The StomachDocument57 pagesTopographic Anatomy and Operative Surgery of The StomachEl Raai El Saleh HospitalPas encore d'évaluation
- Curs Studenti SplinaDocument84 pagesCurs Studenti SplinaAnda Madalina ZahariaPas encore d'évaluation
- Patologia Chirurgicala A Apendicelui CecalDocument7 pagesPatologia Chirurgicala A Apendicelui Cecalnasture_cahcahPas encore d'évaluation
- Chir PedDocument8 pagesChir PedVerde RamonaPas encore d'évaluation
- Week 3Document5 pagesWeek 3AlicePas encore d'évaluation
- 10 KidneysDocument6 pages10 KidneysMark PadulloPas encore d'évaluation
- Congenital Anomaly of PancreasDocument38 pagesCongenital Anomaly of PancreasshalukiriPas encore d'évaluation
- PEDI 2. Embryologic Basis of GI Malformations 2021Document54 pagesPEDI 2. Embryologic Basis of GI Malformations 2021Hayle MaryamPas encore d'évaluation
- Jejunal and Ileal AtresiasDocument37 pagesJejunal and Ileal AtresiasABDUL RAHIM UMAR FAROUKPas encore d'évaluation
- Congenital Development of Urinary SystemDocument31 pagesCongenital Development of Urinary SystemRinxas VerinxtPas encore d'évaluation
- Patologia Chirurgicala A Apendicelui CecalDocument41 pagesPatologia Chirurgicala A Apendicelui CecalIrina DrewPas encore d'évaluation
- Pancreas and SpleenDocument44 pagesPancreas and SpleenOgbuefi PascalPas encore d'évaluation
- Prune Belly SyndromeDocument39 pagesPrune Belly SyndromeHudaPas encore d'évaluation
- Presentacion GastrointestinalDocument228 pagesPresentacion GastrointestinalNb + XB = AVPas encore d'évaluation
- Duodenal ObstructionDocument53 pagesDuodenal ObstructionBoby ChandraPas encore d'évaluation
- Diaphragm: Surgical Anatomy of The DiaphragmDocument14 pagesDiaphragm: Surgical Anatomy of The DiaphragmOlga CerlatPas encore d'évaluation
- Pancreas: Anatomy of The PancreasDocument11 pagesPancreas: Anatomy of The PancreasHart ElettPas encore d'évaluation
- 155 - B3 Sesi 1 Asisten 2015Document91 pages155 - B3 Sesi 1 Asisten 2015Luthfi AnshoriPas encore d'évaluation
- ACUTE ABDOMEN by DR NajamDocument65 pagesACUTE ABDOMEN by DR NajamdasdasfPas encore d'évaluation
- AR - 09 13 - Guimaraes Quencer Part01Document7 pagesAR - 09 13 - Guimaraes Quencer Part01Fernando VerdePas encore d'évaluation
- Surgery of The Bovine Large IntestineDocument18 pagesSurgery of The Bovine Large IntestineJhon Bustamante CanoPas encore d'évaluation
- Gastrointestinal System: Liver Bile Pathways PancreasDocument23 pagesGastrointestinal System: Liver Bile Pathways PancreasTodesengelPas encore d'évaluation
- Terapia Fetala CursDocument70 pagesTerapia Fetala CursGeorgiana Combei UngureanuPas encore d'évaluation
- Ureter AnatomyDocument8 pagesUreter AnatomyGhaly AmirPas encore d'évaluation
- Bowel ObstructionDocument10 pagesBowel Obstructionenke.nwekePas encore d'évaluation
- GIT Abnormality in Infant/Children On Radiology Imaging Which Need Surgery CorrectionDocument48 pagesGIT Abnormality in Infant/Children On Radiology Imaging Which Need Surgery Correctiondr fikriPas encore d'évaluation
- AUGUST 30, 2000 History: A Full Day of Right Upper Quadrant Pain in An Otherwise Healthy Woman. CT Was Performed and Selected Images Are ShownDocument4 pagesAUGUST 30, 2000 History: A Full Day of Right Upper Quadrant Pain in An Otherwise Healthy Woman. CT Was Performed and Selected Images Are ShownAmit Kumar RanoPas encore d'évaluation
- LIEN/SPLEN/LIMPA ReviewDocument36 pagesLIEN/SPLEN/LIMPA ReviewNaomiRimaClaudyaPas encore d'évaluation
- MiniOSCE Surgery 1Document329 pagesMiniOSCE Surgery 1Mohammad BanisalmanPas encore d'évaluation
- Metatarsal Apophysis - Linear and Not FractureDocument14 pagesMetatarsal Apophysis - Linear and Not Fracturenithin shenoiPas encore d'évaluation
- Imperforate Anus and Cloacal MalformationsDocument110 pagesImperforate Anus and Cloacal MalformationsAhmad Abu KushPas encore d'évaluation
- Surgery TacticsDocument154 pagesSurgery TacticsAiman Arifin0% (1)
- 0ac8 PDFDocument17 pages0ac8 PDFRamona MükPas encore d'évaluation
- Samplex PBS 2013Document1 pageSamplex PBS 2013Jen SalutaPas encore d'évaluation
- Gallbladder Anatomy, Physiology, and DiseasesDocument33 pagesGallbladder Anatomy, Physiology, and DiseasesElisha BernabePas encore d'évaluation
- Dr. Asif Mian Ansari DNB Resident Dept. of General Surgery Max Hospital, MohaliDocument25 pagesDr. Asif Mian Ansari DNB Resident Dept. of General Surgery Max Hospital, MohaliKarem Maali100% (1)
- Acute & Chronic PancreatitisDocument26 pagesAcute & Chronic PancreatitisNour AhmededPas encore d'évaluation
- Master Radiology Notes UrologyDocument106 pagesMaster Radiology Notes UrologySafwan ShaikhPas encore d'évaluation
- Anatomie Cai BiliareDocument4 pagesAnatomie Cai BiliareLarisa StanPas encore d'évaluation
- Neonatal Intestinal Obstruction EPSGHAN PDFDocument77 pagesNeonatal Intestinal Obstruction EPSGHAN PDFRobert ChristevenPas encore d'évaluation
- GI System and Abdominal Exam Physical Diagnosis Worksheet: Surface Anatomy / InspectionDocument8 pagesGI System and Abdominal Exam Physical Diagnosis Worksheet: Surface Anatomy / Inspectionrose961Pas encore d'évaluation
- Def - Malformatie A Peretelui Abdominal Anterior-Tulb - de Morfogeneza-InchidereDocument8 pagesDef - Malformatie A Peretelui Abdominal Anterior-Tulb - de Morfogeneza-InchidereBloculTurnPas encore d'évaluation
- Pancreas - Endocrine and Exocrine Functions - Medical LibraryDocument16 pagesPancreas - Endocrine and Exocrine Functions - Medical Libraryjean PiedraPas encore d'évaluation
- Peptic Ulcer Disease: Causes, Symptoms and TreatmentDocument111 pagesPeptic Ulcer Disease: Causes, Symptoms and TreatmentEma RadulescuPas encore d'évaluation
- The PancreasDocument31 pagesThe PancreasAryan DesaiPas encore d'évaluation
- The Pancreas: Anatomy and Clinical ConsiderationsDocument40 pagesThe Pancreas: Anatomy and Clinical ConsiderationsMuthannah MarawanPas encore d'évaluation
- Extra Hepatic Biliary Apparatus ECE: DR - RHS Rajila Professor & HeadDocument29 pagesExtra Hepatic Biliary Apparatus ECE: DR - RHS Rajila Professor & HeadDev SaiPas encore d'évaluation
- Hirschsprung's Disease PathophysiologyDocument8 pagesHirschsprung's Disease Pathophysiologyclaire yowsPas encore d'évaluation
- Colon Anatomy and Appendicitis GuideDocument30 pagesColon Anatomy and Appendicitis GuideKiara GovenderPas encore d'évaluation
- Anatomy StomachDocument43 pagesAnatomy StomachBijo K BennyPas encore d'évaluation
- Anatomy of GALL BLADDER PANCREAS 2016Document32 pagesAnatomy of GALL BLADDER PANCREAS 2016Omar Ali AyoubkhanPas encore d'évaluation
- Exstrophy and Epispadias MedscapeDocument18 pagesExstrophy and Epispadias MedscapeMohammad Rifqi WibowoPas encore d'évaluation
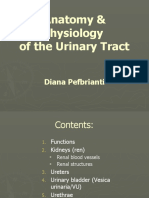
- Anatomy & Physiology URINARY TRACTDocument28 pagesAnatomy & Physiology URINARY TRACTabdullatifPas encore d'évaluation
- Pemeriksaan Rontgen Toraks, Elektrokardiogram (EKG), USG Abdomen Dan EchocardiografiDocument5 pagesPemeriksaan Rontgen Toraks, Elektrokardiogram (EKG), USG Abdomen Dan EchocardiografigorodoePas encore d'évaluation
- Abdominal ExaminationDocument6 pagesAbdominal ExaminationLi FaungPas encore d'évaluation
- Genito-urinary Tract Imaging GuideDocument57 pagesGenito-urinary Tract Imaging GuideAnanya GoswamiPas encore d'évaluation
- Tumors of Pancreas DR DilberDocument51 pagesTumors of Pancreas DR Dilberdrdilber100% (1)
- CLINICAL HISTORY AND DIFFERENTIAL DIAGNOSIS AT YOUR FINGERTIPSD'EverandCLINICAL HISTORY AND DIFFERENTIAL DIAGNOSIS AT YOUR FINGERTIPSPas encore d'évaluation
- Series: Instruction ManualDocument10 pagesSeries: Instruction Manualjbernal89Pas encore d'évaluation
- SikafloorMultiFlexPB-21-certificare OS13Document4 pagesSikafloorMultiFlexPB-21-certificare OS13George EnescuPas encore d'évaluation
- CTT DE LOS ANDES LANGUAGE CENTER WORK GROUP – Waste Disposal reportDocument7 pagesCTT DE LOS ANDES LANGUAGE CENTER WORK GROUP – Waste Disposal reportRosa CapeloPas encore d'évaluation
- Axioms Are Objects, Too - Ontology Engineering Beyond The Modeling of Concepts and RelationsDocument16 pagesAxioms Are Objects, Too - Ontology Engineering Beyond The Modeling of Concepts and RelationsJose Marcelo SchiesslPas encore d'évaluation
- 21 Card CounterDocument56 pages21 Card CounterRosa Meltrozo100% (2)
- Sustainability Relative To The Performance of Buildings: Standard Terminology ForDocument5 pagesSustainability Relative To The Performance of Buildings: Standard Terminology ForEdmundo Jaita CuellarPas encore d'évaluation
- Verb ReviewDocument2 pagesVerb Reviewapi-234410057Pas encore d'évaluation
- WCW - 1993 Training + Contracts 1994Document65 pagesWCW - 1993 Training + Contracts 1994Col. O'NeillPas encore d'évaluation
- Button Attachment SOPDocument22 pagesButton Attachment SOPratno wijaya89% (18)
- Chapter 4Document4 pagesChapter 4KrisTine May LoloyPas encore d'évaluation
- Greater Doha Bus Services: Al Ghanim Bus StationDocument1 pageGreater Doha Bus Services: Al Ghanim Bus Stationramadan rashadPas encore d'évaluation
- Heat Exchangers: DR Ali JawarnehDocument46 pagesHeat Exchangers: DR Ali Jawarnehprasanthi100% (1)
- Deployment of A Self-Expanding Stent Inside An Artery (FEA)Document11 pagesDeployment of A Self-Expanding Stent Inside An Artery (FEA)LogicAndFacts ChannelPas encore d'évaluation
- Solution: Elementary Differential Equations, Section 02, Prof. Loftin, Test 2Document3 pagesSolution: Elementary Differential Equations, Section 02, Prof. Loftin, Test 2DEBASIS SAHOOPas encore d'évaluation
- Desert War Quick Start Guide-Printer FriendlyDocument22 pagesDesert War Quick Start Guide-Printer FriendlyŽeljko ToplekPas encore d'évaluation
- Verbal and Non-VerbalDocument26 pagesVerbal and Non-VerbalDanica ValentinoPas encore d'évaluation
- Carto 3 System OverviewDocument8 pagesCarto 3 System Overviewdanang setiawanPas encore d'évaluation
- Tle-Computer Systems SERVICING (Grade 10) : First Quarter - Module 1 Elements of ComputerDocument9 pagesTle-Computer Systems SERVICING (Grade 10) : First Quarter - Module 1 Elements of ComputerQuerl Manzano SarabiaPas encore d'évaluation
- Subject + Was/were/v II + Object/ComplementDocument6 pagesSubject + Was/were/v II + Object/ComplementRini TiaraPas encore d'évaluation
- Leak Frequency Modelling For Offshore QraDocument9 pagesLeak Frequency Modelling For Offshore QraLuis del BarcoPas encore d'évaluation
- Introducere 1Document11 pagesIntroducere 1Victor EnachiPas encore d'évaluation
- Samson and Delilah (1609-1610) by Peter Paul RubensDocument10 pagesSamson and Delilah (1609-1610) by Peter Paul RubensIoanaMirunaPas encore d'évaluation
- Prices & Services Updates: DashboardDocument1 pagePrices & Services Updates: Dashboardzafira fatimaPas encore d'évaluation
- Ventilator Emvie 9+Document6 pagesVentilator Emvie 9+dedezagita_1_laelyPas encore d'évaluation
- Dilg Memocircular 2023119 - Ca3d912db2Document76 pagesDilg Memocircular 2023119 - Ca3d912db2Korlissemina RascoPas encore d'évaluation
- YÖKDİL HAP KELİME SORULARI WWW - Sinavkampi.com - TRDocument14 pagesYÖKDİL HAP KELİME SORULARI WWW - Sinavkampi.com - TRDemet KöseoğluPas encore d'évaluation
- Apela - Learners - Handbook - L3-L7 - 120721Document34 pagesApela - Learners - Handbook - L3-L7 - 120721shahrol effendy rodziPas encore d'évaluation
- Video ProcessingDocument13 pagesVideo ProcessingChetan B VPas encore d'évaluation
- ITCT - Syllabus - 245052Document8 pagesITCT - Syllabus - 245052Ravi KumarPas encore d'évaluation
- Music Assignment 1Document3 pagesMusic Assignment 1Rubina Devi DHOOMUNPas encore d'évaluation