Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Pre Course MCQ For Doctors November 2014 PDFDocument2 pagesPre Course MCQ For Doctors November 2014 PDFJude Roshan Wijesiri100% (1)
- Propranolol For Infantile Haemangioma: Sandeep Ramkrishna Hambarde, Pradnya Suhas Bendre, Ramdas Dagdu NagargojeDocument2 pagesPropranolol For Infantile Haemangioma: Sandeep Ramkrishna Hambarde, Pradnya Suhas Bendre, Ramdas Dagdu NagargojeJude Roshan WijesiriPas encore d'évaluation
- Algorithms - HyperkalaemiaDocument1 pageAlgorithms - HyperkalaemiaJude Roshan WijesiriPas encore d'évaluation
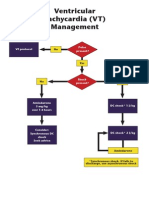
- Ventricular Tachycardia (VT) Management: Pulse Present? VF ProtocolDocument1 pageVentricular Tachycardia (VT) Management: Pulse Present? VF ProtocolJude Roshan WijesiriPas encore d'évaluation
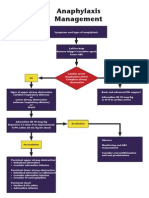
- Algorithms - AnaphylaxisDocument1 pageAlgorithms - AnaphylaxisJude Roshan WijesiriPas encore d'évaluation
- SnakesDocument65 pagesSnakesJude Roshan WijesiriPas encore d'évaluation
- Slma Vaccines Guidelines 2011Document111 pagesSlma Vaccines Guidelines 2011Jude Roshan WijesiriPas encore d'évaluation
- Sri LankaDocument15 pagesSri LankaJude Roshan WijesiriPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Angelie ADocument4 pagesAngelie AMaja TusonPas encore d'évaluation
- Intern Annual16Document7 pagesIntern Annual16Akash PanwarPas encore d'évaluation
- Alternative DietDocument31 pagesAlternative Dietiri_balPas encore d'évaluation
- Actalyke Mini Op Man D6500091JDocument29 pagesActalyke Mini Op Man D6500091Jjyoti ranjanPas encore d'évaluation
- PT - Mapeh 6 - Q4 - V2Document6 pagesPT - Mapeh 6 - Q4 - V2MarlynSanchezTenorioPas encore d'évaluation
- MCQ Pead MockDocument8 pagesMCQ Pead MocknoblefxPas encore d'évaluation
- Act 1 Urinary SystemDocument20 pagesAct 1 Urinary Systemisabellamarie.castillo.crsPas encore d'évaluation
- LipomaDocument51 pagesLipomaAgnes NiyPas encore d'évaluation
- NPB 168 Practice Exam 2Document5 pagesNPB 168 Practice Exam 2Kim Wong100% (1)
- Final Resume Package Douglas ShawDocument3 pagesFinal Resume Package Douglas Shawapi-347691125Pas encore d'évaluation
- E B I W: Safemedicate Rounding Rules GuidelinesDocument9 pagesE B I W: Safemedicate Rounding Rules Guidelineslesky17Pas encore d'évaluation
- Felicias Resume 1Document1 pageFelicias Resume 1api-357153848Pas encore d'évaluation
- ALP Crestline PDFDocument2 pagesALP Crestline PDFJashmyn JagonapPas encore d'évaluation
- Teaching Plan About Conjunctivitis: Haemophilus InfluenzaeDocument3 pagesTeaching Plan About Conjunctivitis: Haemophilus InfluenzaeJanaica Juan100% (1)
- Autonomic Control of The Heart Cardiovascular Reflexes Student Version (7) - 2Document27 pagesAutonomic Control of The Heart Cardiovascular Reflexes Student Version (7) - 2Mohammed MoghavelehPas encore d'évaluation
- Public Notice20oct2014124416 PDFDocument73 pagesPublic Notice20oct2014124416 PDFLeticia RileyPas encore d'évaluation
- Case Study Discretion Advised PDFDocument12 pagesCase Study Discretion Advised PDFGustavo MooriPas encore d'évaluation
- MYDRIATICDocument6 pagesMYDRIATICManik BashaPas encore d'évaluation
- Importance and Applicability of Strotas in Treatment of DiseaseDocument9 pagesImportance and Applicability of Strotas in Treatment of DiseaseAshutosh JhaPas encore d'évaluation
- Faculty 363 Histotechnique Lectures - 2Document27 pagesFaculty 363 Histotechnique Lectures - 2einsteinspy100% (1)
- Ymaa TrainingDocument4 pagesYmaa TraininganattāPas encore d'évaluation
- The PRISMAFLEX System: Making Possible PersonalDocument12 pagesThe PRISMAFLEX System: Making Possible PersonalluisfulaPas encore d'évaluation
- Surgical Correction Subglottic Stenosis of The Larynx: AnnoldDocument6 pagesSurgical Correction Subglottic Stenosis of The Larynx: Annoldcanndy202Pas encore d'évaluation
- Critical Appraisal of Articles About Diagnostic TestsDocument43 pagesCritical Appraisal of Articles About Diagnostic TestshardianPas encore d'évaluation
- Pga 2014 ProspectusDocument31 pagesPga 2014 ProspectusKaranGargPas encore d'évaluation
- Home Remedies Using Onion Prophet666Document2 pagesHome Remedies Using Onion Prophet666Hussainz AliPas encore d'évaluation
- En PIL BetmigaDocument6 pagesEn PIL BetmigaEmma KatePas encore d'évaluation
- Ashkenazi Jewish ScreeningDocument10 pagesAshkenazi Jewish ScreeningJorge SHPas encore d'évaluation
- Induction Update2Document30 pagesInduction Update2yusepPas encore d'évaluation
- Lipoxome Business PresentationDocument20 pagesLipoxome Business PresentationCaerwyn AshPas encore d'évaluation