Vous aimerez peut-être aussi
- Pedia Alhamdollilah FluidsDocument80 pagesPedia Alhamdollilah FluidsArwyn AncogPas encore d'évaluation
- Fluid Management in Neonates and InfantsDocument51 pagesFluid Management in Neonates and InfantsSulabh Shrestha100% (1)
- Fluids, Electrolyte, and Nutrition Management in Neonates: N. Ambalavanan MD Neonatologist October 1998Document40 pagesFluids, Electrolyte, and Nutrition Management in Neonates: N. Ambalavanan MD Neonatologist October 1998gopscharanPas encore d'évaluation
- Fluid Student 2012Document43 pagesFluid Student 2012Sara Ilyas KhanPas encore d'évaluation
- Pediatric Anesthesia (Anesthesia Text) : OpenanesthesiaDocument13 pagesPediatric Anesthesia (Anesthesia Text) : Openanesthesiapradeep danielPas encore d'évaluation
- Case Report DyspepsiaDocument32 pagesCase Report DyspepsiaAnnisa AstariPas encore d'évaluation
- Manajemen Perioperatif Terapi Cairan Pada PediatriDocument35 pagesManajemen Perioperatif Terapi Cairan Pada PediatriZulhendraPas encore d'évaluation
- Pocket Emergency Paediatric CareDocument201 pagesPocket Emergency Paediatric Cares12317100% (2)
- Case Report: Kwashiorkor: BY: JAYA DEV (110100465) Supervisor: Dr. Hj. Tiangsa Sembiring, M.Ked (Ped), Sp.A (K)Document49 pagesCase Report: Kwashiorkor: BY: JAYA DEV (110100465) Supervisor: Dr. Hj. Tiangsa Sembiring, M.Ked (Ped), Sp.A (K)Izaac JdevPas encore d'évaluation
- Pediatric Fluids: Katinka Kersten, MDDocument42 pagesPediatric Fluids: Katinka Kersten, MDSholehuddin MunajjidPas encore d'évaluation
- Tetralogy of Fallot: Supervisor: Dr. Muhammad Ali, Sp.A (K) Presentator: Citra Aryanti 080100050 Marianto 080100112Document48 pagesTetralogy of Fallot: Supervisor: Dr. Muhammad Ali, Sp.A (K) Presentator: Citra Aryanti 080100050 Marianto 080100112Faskanita NadapdapPas encore d'évaluation
- Pediatric SurgeryDocument57 pagesPediatric SurgeryMusekhirPas encore d'évaluation
- Fluids and ElectrolytesDocument70 pagesFluids and ElectrolytesCesar MellaPas encore d'évaluation
- Shock in Children TutorialDocument37 pagesShock in Children TutorialSsenyonga DominicPas encore d'évaluation
- Fluids&LytesDocument33 pagesFluids&LytesMateen ShukriPas encore d'évaluation
- Principles of Neonatal SurgeryDocument44 pagesPrinciples of Neonatal Surgerykbmed2003100% (2)
- Care Plan and Patho Final Feb 25 Left Hip FXDocument16 pagesCare Plan and Patho Final Feb 25 Left Hip FXapi-256360167Pas encore d'évaluation
- Fluids&Lytes PediatricDocument33 pagesFluids&Lytes Pediatricnugraha_esaPas encore d'évaluation
- Pediatric Perioperative MX FinalDocument63 pagesPediatric Perioperative MX FinalHayle MaryamPas encore d'évaluation
- Paediatric Clinical Chemistry: BY DR Okwor C.J Department of Chemical Pathology, UNECDocument41 pagesPaediatric Clinical Chemistry: BY DR Okwor C.J Department of Chemical Pathology, UNECUdochukwu EnebePas encore d'évaluation
- Syok HipovolemikDocument21 pagesSyok HipovolemikIrfandy Chairi Sulaiman LubisPas encore d'évaluation
- Cah 10.01.2018Document26 pagesCah 10.01.2018Emily EresumaPas encore d'évaluation
- Fluid and Electrolyte 10 RDocument87 pagesFluid and Electrolyte 10 RHea YaPas encore d'évaluation
- Perioperative Fluid ManagementDocument123 pagesPerioperative Fluid ManagementAnonymous 86gki5Pas encore d'évaluation
- Fluid ManagementDocument59 pagesFluid ManagementAj Primaditya WardhanaPas encore d'évaluation
- CKDDocument48 pagesCKDJuniorPas encore d'évaluation
- Fluid Dss PKB - RsDocument39 pagesFluid Dss PKB - RsancillaagraynPas encore d'évaluation
- Fluids and Electrolytes PediatricsDocument46 pagesFluids and Electrolytes PediatricsShelley PantinoplePas encore d'évaluation
- Fluid Electrolyte NutritionDocument40 pagesFluid Electrolyte NutritionStrept PneumoniaPas encore d'évaluation
- Paediatric Septic Shock: Corrine BalitDocument37 pagesPaediatric Septic Shock: Corrine BalitJauhari DesloPas encore d'évaluation
- Approach To Ill Looking ChildDocument66 pagesApproach To Ill Looking ChildUzair MuhdPas encore d'évaluation
- Peds Fluid and ElectrolytesDocument12 pagesPeds Fluid and ElectrolytesAshleyPas encore d'évaluation
- Fluid Balance and Venous Access in ChildrenDocument51 pagesFluid Balance and Venous Access in Childrenhayssam rashwan100% (1)
- Diabetic Emergencies Case StudiesDocument32 pagesDiabetic Emergencies Case StudiesLamria Maloni Siahaan0% (1)
- Terapi CairanDocument41 pagesTerapi CairanRatu Qurroh AinPas encore d'évaluation
- Principles+ +LU6Document35 pagesPrinciples+ +LU6Alvin Ray JuanPas encore d'évaluation
- Perioperative Fluid ManagementDocument27 pagesPerioperative Fluid ManagementridhoardiPas encore d'évaluation
- Fluid & ElectrolyteDocument68 pagesFluid & ElectrolytePranay MallPas encore d'évaluation
- 4.fluid and ElectrolytesDocument23 pages4.fluid and ElectrolytesManju KumariPas encore d'évaluation
- Fluid Therapy & Resuscitation I Children (2008 Nov)Document41 pagesFluid Therapy & Resuscitation I Children (2008 Nov)evalPas encore d'évaluation
- CC 9 June 18 Sepsis Neo FixDocument39 pagesCC 9 June 18 Sepsis Neo FixlatifahPas encore d'évaluation
- Perioperative Fluid TherapyDocument36 pagesPerioperative Fluid TherapyUmhy GumianaPas encore d'évaluation
- Case Presentation Aplastic Anamia (Akash Joshi)Document20 pagesCase Presentation Aplastic Anamia (Akash Joshi)Akash JoshiPas encore d'évaluation
- CHP 33 Pediatric CareDocument8 pagesCHP 33 Pediatric CareJeanyanty Yoesteyn DjaranjoeraPas encore d'évaluation
- Management of Paediatric Shock - Fluids and InotropesDocument78 pagesManagement of Paediatric Shock - Fluids and InotropesRahmanu ReztaputraPas encore d'évaluation
- Case MorbiliDocument49 pagesCase MorbiliSiLpi HamidiyahPas encore d'évaluation
- Pediatric Oncology Calculations & Monitoring Clinical PearlsDocument11 pagesPediatric Oncology Calculations & Monitoring Clinical PearlsTaufik HidayahPas encore d'évaluation
- Fluid and ElectrolytesDocument23 pagesFluid and ElectrolytesNanaPas encore d'évaluation
- Neonatal AsphyxiaDocument35 pagesNeonatal Asphyxiaiqiqiqiqiq100% (21)
- Fluids & Electrolytes Imbalance KMUDocument37 pagesFluids & Electrolytes Imbalance KMUSHAFIQPas encore d'évaluation
- Kuliah Infant Periopeative FluidDocument27 pagesKuliah Infant Periopeative FluidMohammad SutamiPas encore d'évaluation
- SAM With DiarrhoeaDocument44 pagesSAM With Diarrhoea7dbnf4stjyPas encore d'évaluation
- Fluid and Electrolyte TherapyDocument4 pagesFluid and Electrolyte TherapyKhirren RaoPas encore d'évaluation
- Fluid Management For The Pediatric Surgical Patient POWERPOINTDocument34 pagesFluid Management For The Pediatric Surgical Patient POWERPOINTDipta Anggara100% (2)
- Gastrointestinal System Disorders For PediaDocument92 pagesGastrointestinal System Disorders For PediaQuolette Constante100% (1)
- Ecf Case StudyDocument54 pagesEcf Case Studyapi-290929891Pas encore d'évaluation
- Fluids and Electrolytes - PaediatricsDocument52 pagesFluids and Electrolytes - PaediatricsZwePas encore d'évaluation
- Health Promotion Throughout The Life Span 7th Edition Edelman Test BankDocument35 pagesHealth Promotion Throughout The Life Span 7th Edition Edelman Test Bankcourtneyharrisbpfyrkateq100% (17)
- Math AA SL P 1 Marks SchemeDocument6 pagesMath AA SL P 1 Marks SchemeMrin GhoshPas encore d'évaluation
- IV. Network Modeling, Simple SystemDocument16 pagesIV. Network Modeling, Simple SystemJaya BayuPas encore d'évaluation
- Scanner and Xcal Comperative Analysis v2Document22 pagesScanner and Xcal Comperative Analysis v2Ziya2009Pas encore d'évaluation
- Data Bulletin Group Motor Installations:: Understanding National Electrical Code (NEC) 430.53 RequirementsDocument8 pagesData Bulletin Group Motor Installations:: Understanding National Electrical Code (NEC) 430.53 RequirementsshoaibPas encore d'évaluation
- Module 1 Notes The White Bird Reading The Image Painting Analysis PDFDocument4 pagesModule 1 Notes The White Bird Reading The Image Painting Analysis PDFMelbely Rose Apigo BaduaPas encore d'évaluation
- Biology Accel Syllabus 2011-2012Document3 pagesBiology Accel Syllabus 2011-2012Mike DeleonPas encore d'évaluation
- Esteem 1999 2000 1.3L 1.6LDocument45 pagesEsteem 1999 2000 1.3L 1.6LArnold Hernández CarvajalPas encore d'évaluation
- Solutions GoldsteinDocument10 pagesSolutions GoldsteinAnyiPas encore d'évaluation
- Presentation - Delight Bulb PDFDocument22 pagesPresentation - Delight Bulb PDFShiva KishorePas encore d'évaluation
- Determination of Drop-Impact Resistance of Plastic BottlesDocument11 pagesDetermination of Drop-Impact Resistance of Plastic BottlesAndres BrañaPas encore d'évaluation
- SSDsDocument3 pagesSSDsDiki Tri IndartaPas encore d'évaluation
- Goliath 90 v129 eDocument129 pagesGoliath 90 v129 eerkanPas encore d'évaluation
- The Broadband ForumDocument21 pagesThe Broadband ForumAnouar AleyaPas encore d'évaluation
- Worksheet Series 5: Answer Any 3 Questions From 1 To 6. (2 Score Each)Document6 pagesWorksheet Series 5: Answer Any 3 Questions From 1 To 6. (2 Score Each)AswithPas encore d'évaluation
- 14p-220 Mud PumpDocument2 pages14p-220 Mud PumpMurali Sambandan50% (2)
- Someone Who Believes in YouDocument1 pageSomeone Who Believes in YouMANOLO C. LUCENECIOPas encore d'évaluation
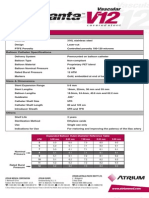
- Advanta V12 Data SheetDocument2 pagesAdvanta V12 Data SheetJuliana MiyagiPas encore d'évaluation
- Table Equivalent Schedule 40 Steel PipeDocument1 pageTable Equivalent Schedule 40 Steel PipeorisPas encore d'évaluation
- 3200AMMe - Part 4Document207 pages3200AMMe - Part 4Tanja Kesic100% (1)
- 300 PSI CTS (MP-1115) Operation Manual Rev1.3Document18 pages300 PSI CTS (MP-1115) Operation Manual Rev1.3Juan Manuel VizosoPas encore d'évaluation
- Sony Cdm82a 82b Cmt-hpx11d Hcd-hpx11d Mechanical OperationDocument12 pagesSony Cdm82a 82b Cmt-hpx11d Hcd-hpx11d Mechanical OperationDanPas encore d'évaluation
- TM-8000 HD Manual PDFDocument37 pagesTM-8000 HD Manual PDFRoxana BirtumPas encore d'évaluation
- Contemporary Philippine Arts From The Regions: Quarter 2 - Module 9 Different Contemporary Art Techniques and PerformanceDocument25 pagesContemporary Philippine Arts From The Regions: Quarter 2 - Module 9 Different Contemporary Art Techniques and PerformanceGrace06 Labin100% (7)
- Hopeless PlacesDocument1 304 pagesHopeless Placesmoreblessingmarvellous659Pas encore d'évaluation
- AoS Soulbound - Pregens - Skyrigger Malgra DainssonDocument2 pagesAoS Soulbound - Pregens - Skyrigger Malgra DainssonAdrien DeschampsPas encore d'évaluation
- Awakened Citizen Programme-Report-class VII-2014Document4 pagesAwakened Citizen Programme-Report-class VII-2014bhsgeneral r m saraswathi50% (4)
- Arduino Oscilloscope ProjectDocument12 pagesArduino Oscilloscope ProjectSathya Narayan100% (1)
- Percent by VolumeDocument19 pagesPercent by VolumeSabrina LavegaPas encore d'évaluation
- Cynosure Starlux 500 Palomar Technical Service ManualDocument47 pagesCynosure Starlux 500 Palomar Technical Service ManualJF SilvaPas encore d'évaluation