Vous aimerez peut-être aussi
- Colloidal Silver Cures MRSA ReportDocument16 pagesColloidal Silver Cures MRSA ReportGodwinPas encore d'évaluation
- Provisional Restoration Options in Implant DentistryDocument8 pagesProvisional Restoration Options in Implant Dentistrydevendra chhonkarPas encore d'évaluation
- Fundamentals and Applications of Controlled Release Drug Delivery PDFDocument607 pagesFundamentals and Applications of Controlled Release Drug Delivery PDFTurco Sekoof50% (2)
- NCP Post DebridementDocument7 pagesNCP Post Debridementtintinlovessu100% (2)
- Acute Coronary Syndrome 052014Document91 pagesAcute Coronary Syndrome 052014Fatahillah NazarPas encore d'évaluation
- Soal Blok 13Document13 pagesSoal Blok 13daniimamPas encore d'évaluation
- Seminar OverdentureDocument73 pagesSeminar OverdentureNisha GargPas encore d'évaluation
- Acut Coronary Syndrome: Joko Sutrisno, S.Kep, NsDocument54 pagesAcut Coronary Syndrome: Joko Sutrisno, S.Kep, NsJokoSutrisnoPas encore d'évaluation
- Communicable Disease SurveillanceDocument60 pagesCommunicable Disease SurveillanceAmeer MuhammadPas encore d'évaluation
- Anatomi JantungDocument54 pagesAnatomi JantungsaifudinPas encore d'évaluation
- Case Report Hemorrhoids: Preceptor: Dr. Dr. Bambang Arianto SP.B FinacsDocument22 pagesCase Report Hemorrhoids: Preceptor: Dr. Dr. Bambang Arianto SP.B FinacsTetipuspita SariPas encore d'évaluation
- Anesthesiology MnemonicsDocument1 pageAnesthesiology MnemonicsMartin Susanto, MD100% (3)
- 2016 Revised Standards For Clinical Dental Hygiene PracticeDocument16 pages2016 Revised Standards For Clinical Dental Hygiene PracticeElvira PurnamasariPas encore d'évaluation
- Skrinning Karsinoma ServiksDocument33 pagesSkrinning Karsinoma ServiksnowemgfPas encore d'évaluation
- Shock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentDocument64 pagesShock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentHarika BandaruPas encore d'évaluation
- IntussusceptionDocument10 pagesIntussusceptionPatrick DycocoPas encore d'évaluation
- Obat THTDocument5 pagesObat THTFelicia Puspita SariPas encore d'évaluation
- Patofisiologi BatukDocument53 pagesPatofisiologi BatukGd PadmawijayaPas encore d'évaluation
- Death Case Dr. MeikoDocument49 pagesDeath Case Dr. MeikoMohamad ZulfikarPas encore d'évaluation
- 2 DHF InternaDocument59 pages2 DHF Internasaladass 2Pas encore d'évaluation
- Diabetic FootDocument73 pagesDiabetic Footmohammad.irfanPas encore d'évaluation
- THT Bimbel Ukdi Mantap 2015 - NorestrictionDocument227 pagesTHT Bimbel Ukdi Mantap 2015 - NorestrictionpanduPas encore d'évaluation
- DyspneaDocument34 pagesDyspneaAlvin BrilianPas encore d'évaluation
- Anemia E.C Hematemesis Melena E.C Suspect Gastritis ErrosiveDocument37 pagesAnemia E.C Hematemesis Melena E.C Suspect Gastritis ErrosiveAndayanaIdhamPas encore d'évaluation
- Bilas LambungDocument12 pagesBilas LambungNthie UnguPas encore d'évaluation
- Cme Acs 2. Stemi (Izzah)Document36 pagesCme Acs 2. Stemi (Izzah)Hakimah K. SuhaimiPas encore d'évaluation
- Lapkas 4 - Pneumonia Susp. Covid 19-Fenda KhafidhotentyDocument17 pagesLapkas 4 - Pneumonia Susp. Covid 19-Fenda KhafidhotentydianarahimmPas encore d'évaluation
- Baca Dari PapdiDocument4 pagesBaca Dari PapdiAriane BeninaPas encore d'évaluation
- Pembahasan TO 3 Agustus 15 PDFDocument802 pagesPembahasan TO 3 Agustus 15 PDFFahmi Afif AlbonehPas encore d'évaluation
- Resusitasi NeonatusDocument22 pagesResusitasi NeonatusnikkitaihsanPas encore d'évaluation
- Kegawatan Respirasi May2016-FkumyDocument62 pagesKegawatan Respirasi May2016-FkumyAgustina Tri P. DPas encore d'évaluation
- Anaesthesia SummaryDocument36 pagesAnaesthesia SummaryRazan QassemPas encore d'évaluation
- Refreshing DHFDocument13 pagesRefreshing DHFNia Nurhayati ZakiahPas encore d'évaluation
- Acute AbdomenDocument42 pagesAcute AbdomenErika Agustina KasdjonoPas encore d'évaluation
- Eloesser Flap Thoracostomy WindowDocument20 pagesEloesser Flap Thoracostomy WindowJEFFRI JEFFRIPas encore d'évaluation
- Tehnik - Tehnik Analgesia Post OperasiDocument32 pagesTehnik - Tehnik Analgesia Post OperasiGuntur Aryo PuntodewoPas encore d'évaluation
- Cervical Spine InjuriesDocument18 pagesCervical Spine InjuriesAnnapurna DangetiPas encore d'évaluation
- Maternal Resuscitation DrillDocument23 pagesMaternal Resuscitation Drillapi-219741636100% (2)
- Air Way Management (ABCDE of Trauma)Document25 pagesAir Way Management (ABCDE of Trauma)makmmkaPas encore d'évaluation
- CR DR - Dedi Hidropneumothorax Ec TB ParuDocument38 pagesCR DR - Dedi Hidropneumothorax Ec TB ParuBunga Listia ParamitaPas encore d'évaluation
- Jumlah Tetesan Infus MakroDocument2 pagesJumlah Tetesan Infus MakroMamanya Ef Taya ThalitaPas encore d'évaluation
- Askep MCI - AchirmanDocument53 pagesAskep MCI - AchirmanmarthaPas encore d'évaluation
- Prof - Dr. Ruswan Dachlan, SP An KIC Dept - of Anaesthesiology & Intensive Care FKUIDocument71 pagesProf - Dr. Ruswan Dachlan, SP An KIC Dept - of Anaesthesiology & Intensive Care FKUIFerdy ErawanPas encore d'évaluation
- Shock ManagementDocument14 pagesShock ManagementnataliaPas encore d'évaluation
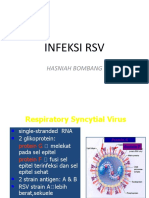
- Infeksi RSV: Hasniah BombangDocument12 pagesInfeksi RSV: Hasniah Bombangmuh hardiansyahPas encore d'évaluation
- Status Epileptikus Morning ReportDocument16 pagesStatus Epileptikus Morning Reportlie antoPas encore d'évaluation
- Print RapiDocument32 pagesPrint RapiNiedlichta TamaPas encore d'évaluation
- Colour of UrineDocument1 pageColour of Urinetmunroe961Pas encore d'évaluation
- Acute Diffuse Otitis ExternaDocument36 pagesAcute Diffuse Otitis ExternaIlham Isnin Dolyanov HasibuanPas encore d'évaluation
- DEMAM Pada Bayi Dan Anak UmyDocument40 pagesDEMAM Pada Bayi Dan Anak UmyFarika NorPas encore d'évaluation
- Batu Saluran Kemih: Dr. Suhaemi, SPPD, FinasimDocument57 pagesBatu Saluran Kemih: Dr. Suhaemi, SPPD, FinasimAfri AdiPas encore d'évaluation
- Journal ReadingDocument18 pagesJournal ReadingnafisyarifahPas encore d'évaluation
- Skdi GehDocument30 pagesSkdi GehviandamayantiPas encore d'évaluation
- Jurus Andalan Bedah 3Document20 pagesJurus Andalan Bedah 3fardan chaisarPas encore d'évaluation
- Hypospadias: Case ReportDocument24 pagesHypospadias: Case Reportbudi haryadiPas encore d'évaluation
- CBD Hilman Suhaili (Dr. Saugi SP - PD, KKV)Document40 pagesCBD Hilman Suhaili (Dr. Saugi SP - PD, KKV)HiLmanPas encore d'évaluation
- Pembahasan UKDI CLINIC 1 Batch Mei 2016Document535 pagesPembahasan UKDI CLINIC 1 Batch Mei 2016William Hartanto RusliPas encore d'évaluation
- Initial Assessment: - Rambam Medical Center - DR Nordkin DmitriDocument60 pagesInitial Assessment: - Rambam Medical Center - DR Nordkin Dmitridheviant12Pas encore d'évaluation
- Anatomi Dan Histologi Saluran Cerna BawahDocument20 pagesAnatomi Dan Histologi Saluran Cerna BawahIlhamDevirxaPas encore d'évaluation
- Krisis Tiroid FixDocument38 pagesKrisis Tiroid FixVita DesriantiPas encore d'évaluation
- Syok Kardiogenik E.C. Sindrom Koroner Akut: Dr. Sarah QonitahDocument43 pagesSyok Kardiogenik E.C. Sindrom Koroner Akut: Dr. Sarah QonitahAnti TjahyaPas encore d'évaluation
- Cairan CaseDocument7 pagesCairan CaseBryan HoriandoPas encore d'évaluation
- Cor Pulmonale Chronicum (CPC) : Bedside TeachingDocument7 pagesCor Pulmonale Chronicum (CPC) : Bedside Teachingaji2703Pas encore d'évaluation
- SDL Obat EmergencyDocument26 pagesSDL Obat EmergencyfarhantunichiaPas encore d'évaluation
- AKI & Indikasi CRRTDocument25 pagesAKI & Indikasi CRRTMaya Sari BaharumPas encore d'évaluation
- MORNING REPORT Ipd 040914Document22 pagesMORNING REPORT Ipd 040914Teddy PrawiroPas encore d'évaluation
- Morning Report: June 6, 2013Document17 pagesMorning Report: June 6, 2013Ayu KristinaPas encore d'évaluation
- Morning Report 3rd Aprl 2014Document25 pagesMorning Report 3rd Aprl 2014hazelelPas encore d'évaluation
- Post Partum Ischemic Stroke About A CaseDocument2 pagesPost Partum Ischemic Stroke About A CaseInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Respiratory Distress SyndromeDocument7 pagesRespiratory Distress SyndromeBilal RowaihiPas encore d'évaluation
- DCVMN Protocol - Version 1.0 - Dated 14th April 2023Document42 pagesDCVMN Protocol - Version 1.0 - Dated 14th April 2023gunjan.guptaPas encore d'évaluation
- Fasciolopsis BuskiDocument18 pagesFasciolopsis BuskiAmritesh KumarPas encore d'évaluation
- Surveillance Guide For Vaccine-Preventable Diseases in The WHO South-East Asia RegionDocument28 pagesSurveillance Guide For Vaccine-Preventable Diseases in The WHO South-East Asia RegionDebPas encore d'évaluation
- Ally Treated Teeth As AbutmentsDocument6 pagesAlly Treated Teeth As AbutmentsLodi Al-SayedPas encore d'évaluation
- National Tuberculosis Control ProgramDocument37 pagesNational Tuberculosis Control Programjava lattePas encore d'évaluation
- Location of First Aid Kit OnboardDocument1 pageLocation of First Aid Kit OnboardLoyd Christian MoradaPas encore d'évaluation
- CircumcisionDocument7 pagesCircumcisionChioma OkoPas encore d'évaluation
- Monitoring Terapi Obat Dalam Pharmaceutical CareDocument55 pagesMonitoring Terapi Obat Dalam Pharmaceutical CareMaya ngoyemPas encore d'évaluation
- Baird 2017Document20 pagesBaird 2017Jhasmyn MartinezPas encore d'évaluation
- Day 15 Short Writing - 1Document1 pageDay 15 Short Writing - 1Internship Reports BdPas encore d'évaluation
- AlexionDocument2 pagesAlexionLiz HartPas encore d'évaluation
- International Recruitment Application Form (New)Document5 pagesInternational Recruitment Application Form (New)EL SHITAPas encore d'évaluation
- Facts: Legal Medicine - Medical Negligence Digest by Bianca Beltran 1Document115 pagesFacts: Legal Medicine - Medical Negligence Digest by Bianca Beltran 1Caryl Angela SalesPas encore d'évaluation
- Daftar PustakaDocument3 pagesDaftar PustakaPrama GitaPas encore d'évaluation
- CGH:2018 09 13:maravillaDocument3 pagesCGH:2018 09 13:maravillaRachelle MaravillaPas encore d'évaluation
- Community PharmacyDocument2 pagesCommunity PharmacyChandra SarathPas encore d'évaluation
- Maternal and Child Nursing Answers and RationaleDocument94 pagesMaternal and Child Nursing Answers and RationaleAnn Michelle Tarrobago100% (1)
- Manipur Neet Ug Qualified Candidates ListDocument24 pagesManipur Neet Ug Qualified Candidates ListDenovo WangPas encore d'évaluation
- Orthodontic Clinical Case PresentationDocument47 pagesOrthodontic Clinical Case Presentationaung NaingmyoPas encore d'évaluation
- Resume-Jennifer BarnettDocument2 pagesResume-Jennifer Barnettapi-258915393Pas encore d'évaluation