Vous aimerez peut-être aussi
- General Concepts of Growth &developmentDocument107 pagesGeneral Concepts of Growth &developmentNeelima ChandranPas encore d'évaluation
- 1.G&D-basic Concepts NewDocument35 pages1.G&D-basic Concepts NewYuvashreePas encore d'évaluation
- Biological DevelopmentDocument48 pagesBiological DevelopmentDaph P. EchanePas encore d'évaluation
- Developmental Milestones PresentationDocument154 pagesDevelopmental Milestones PresentationMark Jaco AngPas encore d'évaluation
- Anthro Unit 10Document30 pagesAnthro Unit 10Sanjana IASPas encore d'évaluation
- 1.postnatal Growth and DevelopmentDocument135 pages1.postnatal Growth and DevelopmentAJPEDO LIFEPas encore d'évaluation
- Theories of GrowthDocument33 pagesTheories of GrowthMaitreye PriyadarshiniPas encore d'évaluation
- Ortho SwapnaDocument50 pagesOrtho SwapnaSwapnagandha R KatePas encore d'évaluation
- L.E.T Child & Adolescent Dev.Document109 pagesL.E.T Child & Adolescent Dev.Marlon BalictarPas encore d'évaluation
- Growth Pattern, Variability and Timing in OrthodonticsDocument112 pagesGrowth Pattern, Variability and Timing in OrthodonticsEmad Ahmad Anis67% (3)
- Ontogenesis of Man: From Conception to Adulthood and to His Final DestinationD'EverandOntogenesis of Man: From Conception to Adulthood and to His Final DestinationPas encore d'évaluation
- UNIT II Growth & DevelopmemtDocument110 pagesUNIT II Growth & DevelopmemtSifanaPas encore d'évaluation
- Il,.m F) x57 !8uqz.Document5 pagesIl,.m F) x57 !8uqz.Charles JosePas encore d'évaluation
- Development Across The Lifespan: by Priscilla MugambiDocument50 pagesDevelopment Across The Lifespan: by Priscilla MugambiCalvin CaltotoPas encore d'évaluation
- A Study On Various Factors Affecting Growth During The First Two Years of LifeDocument22 pagesA Study On Various Factors Affecting Growth During The First Two Years of LifeesycosminPas encore d'évaluation
- PEAK HEIGHT VELOCITY OF GROWTHDocument35 pagesPEAK HEIGHT VELOCITY OF GROWTHNeeraj AroraPas encore d'évaluation
- Understanding Facial Growth & DevelopmentDocument74 pagesUnderstanding Facial Growth & DevelopmentSubhashini RajshekarPas encore d'évaluation
- Week 1Document62 pagesWeek 1Reentsha EllyPas encore d'évaluation
- Determinants of Human BehaviorDocument67 pagesDeterminants of Human BehaviorMARK EVANSPas encore d'évaluation
- The Child and Adolescent Learners and Learning PrinciplesDocument6 pagesThe Child and Adolescent Learners and Learning Principlesrizzamae belenPas encore d'évaluation
- Child and Adolescent Development in LearningDocument54 pagesChild and Adolescent Development in LearningKwame KakariPas encore d'évaluation
- Growth and DevelopmentDocument62 pagesGrowth and DevelopmentSmritikana MarjitPas encore d'évaluation
- Unit 3 Different Stages of Human Development: 3.0 ObjectivesDocument27 pagesUnit 3 Different Stages of Human Development: 3.0 ObjectivesLuciennePas encore d'évaluation
- FACTORS AFFECTING GROWTH AND DEVELOPMENT by NavarroDocument5 pagesFACTORS AFFECTING GROWTH AND DEVELOPMENT by NavarroShereen AlobinayPas encore d'évaluation
- Growth and DevelopmentDocument116 pagesGrowth and DevelopmentKavipriya100% (1)
- Child and Adolescent 2nd YearDocument9 pagesChild and Adolescent 2nd Yearshussettebecondal91821Pas encore d'évaluation
- Craniofacial Growth and DevelopmentDocument42 pagesCraniofacial Growth and DevelopmentDegoma, Mary NoelynPas encore d'évaluation
- Lecture 3 Physical Development: Dr. LIN DanDocument44 pagesLecture 3 Physical Development: Dr. LIN DanNick AviationPas encore d'évaluation
- Child and Adolescent Development (COMPILATION)Document115 pagesChild and Adolescent Development (COMPILATION)Troy Silverio62% (13)
- PsychreportDocument9 pagesPsychreportPoppy MargoPas encore d'évaluation
- Physical Growth, Maturation and Aging: Francis FrimpongDocument30 pagesPhysical Growth, Maturation and Aging: Francis FrimpongFrancis FrimpongPas encore d'évaluation
- Human Growth SEM-01 - A1Document85 pagesHuman Growth SEM-01 - A1ggsachary100% (1)
- Developing Through The Life Span: Learning ObjectivesDocument18 pagesDeveloping Through The Life Span: Learning ObjectivesHayaton IRPas encore d'évaluation
- Developing Through The Life SpanDocument11 pagesDeveloping Through The Life SpanMa. Nenita L. MagallanesPas encore d'évaluation
- BA Psychology Sem IIIDocument176 pagesBA Psychology Sem IIIsaravanankingmaker301Pas encore d'évaluation
- Concepts of Growth and Development in DentistryDocument43 pagesConcepts of Growth and Development in DentistryWillan JumboPas encore d'évaluation
- The Stages of Human DevelopmentDocument53 pagesThe Stages of Human DevelopmentMay BañezPas encore d'évaluation
- Growth and DevelopmentDocument163 pagesGrowth and DevelopmentGeethanjali SadasivamPas encore d'évaluation
- Human Growth & Development from womb to tombDocument47 pagesHuman Growth & Development from womb to tombFrancisco GomezPas encore d'évaluation
- Child and Adolescent DevelopmentDocument288 pagesChild and Adolescent DevelopmentHann alvarezPas encore d'évaluation
- Basic Concepts in Child and Adolescent Development: Mr. Rodel Bryan C. ValdezDocument22 pagesBasic Concepts in Child and Adolescent Development: Mr. Rodel Bryan C. ValdezJessica Nisperos EspenillaPas encore d'évaluation
- Ilmu Ternak Potong Dan Kerja Minggu 7Document152 pagesIlmu Ternak Potong Dan Kerja Minggu 7yahya arifPas encore d'évaluation
- Current Research and Pedagogical Applications On Biological DevelopmentDocument11 pagesCurrent Research and Pedagogical Applications On Biological DevelopmentFaye LannaPas encore d'évaluation
- ECE 103 Updated Handout 2023Document26 pagesECE 103 Updated Handout 2023Jevelyn Lagumbay AntecamaraPas encore d'évaluation
- Assignment 1 EDU 302 Human Development and Learning Fall 2020Document4 pagesAssignment 1 EDU 302 Human Development and Learning Fall 2020Waqar Bin AmeenPas encore d'évaluation
- Courage Is What It Takes To Stand Up and Speak But Courage Is Also What It Takes To Sit Down and ListenDocument28 pagesCourage Is What It Takes To Stand Up and Speak But Courage Is Also What It Takes To Sit Down and ListenKewkew AzilearPas encore d'évaluation
- Growth and DevelopmentDocument10 pagesGrowth and DevelopmentPiyush DuttaPas encore d'évaluation
- EDUC101Document5 pagesEDUC101Zairah AgustinPas encore d'évaluation
- CBSE Class 11 Psychology Chapter 4Document20 pagesCBSE Class 11 Psychology Chapter 4Zahid GolandazPas encore d'évaluation
- EP - Chapter TwoDocument16 pagesEP - Chapter TwoBesufikad ShiferawPas encore d'évaluation
- Growth - Principles and ConceptsDocument70 pagesGrowth - Principles and ConceptsPranaliPas encore d'évaluation
- Physiology Child Growth and Development: Prof - Dr. H.Gusbakti, MSC, PKK, AifmDocument92 pagesPhysiology Child Growth and Development: Prof - Dr. H.Gusbakti, MSC, PKK, AifmEcha Rianti SosantaPas encore d'évaluation
- Lovely Professional University: TopicDocument17 pagesLovely Professional University: Topicladdi4uPas encore d'évaluation
- DEVBIO Introduction - Lecture NotesDocument4 pagesDEVBIO Introduction - Lecture NotesAyako HayashidaPas encore d'évaluation
- DevPsych ReviewerDocument11 pagesDevPsych ReviewerOdiesa faye CanonigoPas encore d'évaluation
- Lecture 7 - Child Development TheoriesDocument16 pagesLecture 7 - Child Development TheoriesЖеня МатееваPas encore d'évaluation
- Growth and Development 6th Week - 025146Document5 pagesGrowth and Development 6th Week - 025146Adeuyi VictorPas encore d'évaluation
- Nutritional Anthropological Physical Development Clinical Characteristics and Biochemical Parameters Among ChildrenD'EverandNutritional Anthropological Physical Development Clinical Characteristics and Biochemical Parameters Among ChildrenPas encore d'évaluation
- Human Body Systems: Nervous /Muscles/Skeleton SystemsDocument32 pagesHuman Body Systems: Nervous /Muscles/Skeleton SystemsWilver James Satinitigan NeriPas encore d'évaluation
- 1 - Anatomy of The KidneyDocument15 pages1 - Anatomy of The Kidneysara khanPas encore d'évaluation
- Medical Physiology Membrane PotentialsDocument39 pagesMedical Physiology Membrane PotentialssanggetharPas encore d'évaluation
- Lateral Wall of NoseDocument11 pagesLateral Wall of NoseaparnajechuPas encore d'évaluation
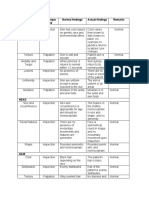
- Area Assessed Technique Used Normal Findings Actual Findings Remarks SkinDocument6 pagesArea Assessed Technique Used Normal Findings Actual Findings Remarks SkinLadybelle GototosPas encore d'évaluation
- Brain Review JeopardyDocument51 pagesBrain Review Jeopardyapi-261267976Pas encore d'évaluation
- HEMATOLOGYDocument36 pagesHEMATOLOGYMA. ANDREA NICOLE BITOINPas encore d'évaluation
- Human ReproductionDocument20 pagesHuman ReproductionKhibul Lim100% (1)
- DentinDocument89 pagesDentinDr Zadeno kithanPas encore d'évaluation
- Female Reproductive AnatomydDocument7 pagesFemale Reproductive AnatomydOneda Ganbatte' KudasaiPas encore d'évaluation
- Hem - Lab 4 Retic - 09Document9 pagesHem - Lab 4 Retic - 09djebrutPas encore d'évaluation
- Bone HealingDocument7 pagesBone HealingArfan PrawiragaraPas encore d'évaluation
- Exercise 11 Activity 1Document4 pagesExercise 11 Activity 1MEGAN NICOLE PERNILLA HERNANDEZPas encore d'évaluation
- Assessing the Abdomen: 4 Quadrants and 9 RegionsDocument54 pagesAssessing the Abdomen: 4 Quadrants and 9 RegionsWilma Acorin OrillinedaPas encore d'évaluation
- Year 4 Reading Your Digestive SystemDocument11 pagesYear 4 Reading Your Digestive SystemMa Donabel LopezPas encore d'évaluation
- Duke University - Medical Neuroscience - by Leonard E. White, Ph.D.Document16 pagesDuke University - Medical Neuroscience - by Leonard E. White, Ph.D.Ejogheneta OnojakePas encore d'évaluation
- Comparing Prokaryotic and Eukaryotic CellsDocument94 pagesComparing Prokaryotic and Eukaryotic CellsTrevannie EdwardsPas encore d'évaluation
- Surgical Report - MRMDocument4 pagesSurgical Report - MRMapi-551638506Pas encore d'évaluation
- 1999-Identification and Function of The Centrosome CentromatrixDocument10 pages1999-Identification and Function of The Centrosome CentromatrixyicinenPas encore d'évaluation
- Throwing Biomechanics BreakdownDocument7 pagesThrowing Biomechanics Breakdownarold bodoPas encore d'évaluation
- What living things are made of cells, tissues, organs and systemsDocument10 pagesWhat living things are made of cells, tissues, organs and systemsRamyRamia ElzantPas encore d'évaluation
- Medical Terminology For Dummies Cheat SheetDocument5 pagesMedical Terminology For Dummies Cheat SheetSir SunePas encore d'évaluation
- Reticular FormationDocument26 pagesReticular Formationsr_sushilPas encore d'évaluation
- Biology of Human Reproductive SystemDocument51 pagesBiology of Human Reproductive Systemlen lehangPas encore d'évaluation
- Male Reproductive System CanvaDocument35 pagesMale Reproductive System CanvaDex VargasPas encore d'évaluation
- Anes Airway-IntubationDocument12 pagesAnes Airway-IntubationSGD5Christine MendozaPas encore d'évaluation
- Female Reproductive Organ GuideDocument19 pagesFemale Reproductive Organ Guidemistry100% (1)
- Activity No. 7.1 BloodDocument2 pagesActivity No. 7.1 BloodDree SermanPas encore d'évaluation
- Foetal Membrane and Amniotic Fluid FunctionsDocument10 pagesFoetal Membrane and Amniotic Fluid FunctionsN. SivaPas encore d'évaluation
- Animal Tissues WorksheetDocument8 pagesAnimal Tissues WorksheetMaxene LuisPas encore d'évaluation