Vous aimerez peut-être aussi
- EMQ Samples MicrobiologyDocument5 pagesEMQ Samples MicrobiologyHugh JacobsPas encore d'évaluation
- Case Study CLD 1Document12 pagesCase Study CLD 1MoonPas encore d'évaluation
- Airway Management - AdultDocument13 pagesAirway Management - AdultD M Shawkot HossainPas encore d'évaluation
- Renal CalculusDocument34 pagesRenal CalculusChandrashekar N.k.Pas encore d'évaluation
- Urolithiasis SeminarDocument50 pagesUrolithiasis SeminarSiddharth GuptaPas encore d'évaluation
- Renal Calculi & Ureteric Calculi: DR Surajit LahiriDocument27 pagesRenal Calculi & Ureteric Calculi: DR Surajit LahiriJaymalya100% (4)
- Urolithiasis - Modified LectureDocument35 pagesUrolithiasis - Modified Lecturemarina_shawkyPas encore d'évaluation
- Renal Calculi IntroductionDocument4 pagesRenal Calculi IntroductionirysatherfinestPas encore d'évaluation
- Renal CalculiDocument30 pagesRenal CalculiAnaiah Jaaziel KhanPas encore d'évaluation
- Acute Renal Failure: Dr. Bobi Ahmad S, S.KPDocument62 pagesAcute Renal Failure: Dr. Bobi Ahmad S, S.KPdr.Bobi Ahmad Sahid, S.KepPas encore d'évaluation
- HydronephrosisDocument7 pagesHydronephrosisNaqash NoblePas encore d'évaluation
- Jaundice: DR: Ramy A. SamyDocument42 pagesJaundice: DR: Ramy A. Samyoscar3spurgeonPas encore d'évaluation
- CholelithiasisDocument65 pagesCholelithiasisGAURAV0% (1)
- Renal CalculiDocument5 pagesRenal CalculiRufus Raj100% (1)
- Anorectal MalformationsDocument6 pagesAnorectal Malformationskhadzx100% (2)
- HypernatremiaDocument7 pagesHypernatremiaNader Smadi100% (1)
- Kidney CancerDocument31 pagesKidney CancerEfren Elico VenguaPas encore d'évaluation
- Liver AbscessDocument15 pagesLiver AbscessAli Aborges Jr.Pas encore d'évaluation
- Pyothorax / Purulent Pleuritis / Empyema Thoracis: Prepared By: Sharmin SusiwalaDocument22 pagesPyothorax / Purulent Pleuritis / Empyema Thoracis: Prepared By: Sharmin SusiwalaAnkan Dey100% (1)
- Anaphylactic ShockDocument14 pagesAnaphylactic ShockAuliya AndiPas encore d'évaluation
- Anal Canal: Fissure in Ano HaemorrhoidsDocument37 pagesAnal Canal: Fissure in Ano Haemorrhoidsyash shrivastavaPas encore d'évaluation
- Hiatal Hernia AchalasiaDocument22 pagesHiatal Hernia AchalasiaDhen MarcPas encore d'évaluation
- Portal HypertensionDocument23 pagesPortal HypertensionSumathi GopinathPas encore d'évaluation
- Renal StoneDocument8 pagesRenal Stonevirz23Pas encore d'évaluation
- Heparin Induced ThrombocytopeniaDocument29 pagesHeparin Induced Thrombocytopeniahari krishna100% (6)
- Renal Calculi (NS Presentation)Document24 pagesRenal Calculi (NS Presentation)Norsyakira NawirPas encore d'évaluation
- Gout N Osteoporasis GaganDocument33 pagesGout N Osteoporasis GaganGaganpreet KaurPas encore d'évaluation
- HematuriaDocument42 pagesHematuriaWasim R. IssaPas encore d'évaluation
- Colon Cancer: Risk FactorsDocument3 pagesColon Cancer: Risk FactorsAshley VillanuevaPas encore d'évaluation
- Renal Trauma: Dr. Mars Dwi Tjahjo, Sp.UDocument21 pagesRenal Trauma: Dr. Mars Dwi Tjahjo, Sp.UbayuPas encore d'évaluation
- Anatomy & PhysiologyDocument9 pagesAnatomy & Physiologyrachael80% (5)
- Renal TumorsDocument38 pagesRenal TumorsMim Rashed0% (1)
- Inguinal Hernias and Abdominal Wall Defects: Murad Nuserat & Abd AL-Rahman AlhelwDocument51 pagesInguinal Hernias and Abdominal Wall Defects: Murad Nuserat & Abd AL-Rahman AlhelwRashed ShatnawiPas encore d'évaluation
- Cholelithiasis GallstoneDocument22 pagesCholelithiasis GallstoneBheru LalPas encore d'évaluation
- Cholelithiasis: Group MembersDocument12 pagesCholelithiasis: Group MembersShiela GutierrezPas encore d'évaluation
- Cholelithiasis When They Are in The Bile CholedocolithiasisDocument15 pagesCholelithiasis When They Are in The Bile Choledocolithiasishisabumohamed100% (1)
- Intestinal ObstructionDocument12 pagesIntestinal ObstructionNurul Nurnita100% (1)
- Renal FailureDocument41 pagesRenal Failure12046Pas encore d'évaluation
- Gastrointestinal EndosDocument28 pagesGastrointestinal EndosAqeel AhmedPas encore d'évaluation
- Development of Hemorrhoids: Anal Canal AnatomyDocument20 pagesDevelopment of Hemorrhoids: Anal Canal AnatomyKris TejereroPas encore d'évaluation
- Chronic Renal FailureDocument14 pagesChronic Renal FailureyazzzPas encore d'évaluation
- Biliary Tree LectureDocument58 pagesBiliary Tree Lecturesgod34Pas encore d'évaluation
- Anal FistulaDocument26 pagesAnal FistulaBeverly PagcaliwaganPas encore d'évaluation
- Varicose Vein FinalDocument60 pagesVaricose Vein FinalblitheleevsPas encore d'évaluation
- PancreatitisDocument59 pagesPancreatitisAarif RanaPas encore d'évaluation
- Anemia IntroductionDocument15 pagesAnemia IntroductionNitesh Kotian100% (1)
- Rectal ExaminationDocument21 pagesRectal ExaminationdrgbkhanPas encore d'évaluation
- Risk Factors: CholelithiasisDocument10 pagesRisk Factors: CholelithiasisRoyster CabralPas encore d'évaluation
- 6 PneumothoraxDocument25 pages6 PneumothoraxRana VandanaPas encore d'évaluation
- CHOLELITHIASISSDocument29 pagesCHOLELITHIASISSAngelica Mercado SirotPas encore d'évaluation
- Splints and Tractions in OrthopaedicsDocument26 pagesSplints and Tractions in OrthopaedicsArun C RajPas encore d'évaluation
- ThyrotoxicosisDocument42 pagesThyrotoxicosisShaw Khan100% (7)
- Cholelithiasis: - Other Names: - Gallbladder Attack - Biliary Colic - Gallstone Attack - Bile Calculus - Biliary CalculusDocument101 pagesCholelithiasis: - Other Names: - Gallbladder Attack - Biliary Colic - Gallstone Attack - Bile Calculus - Biliary CalculusYvonne100% (1)
- Abdominal Compartment SyndromeDocument24 pagesAbdominal Compartment SyndromePrateek Vaswani100% (1)
- Management of OliguriaDocument14 pagesManagement of OliguriaAhmed El-MalkyPas encore d'évaluation
- Peptic Ulcer DiseaseDocument18 pagesPeptic Ulcer DiseasechetankumarbhumireddyPas encore d'évaluation
- Cirrhosis of LiverDocument35 pagesCirrhosis of LiverShazia Parveen100% (1)
- Case Pres HydronephrosisDocument39 pagesCase Pres HydronephrosisLouie Dela Cruz100% (3)
- Liver CancerDocument1 pageLiver CancerTarantado67% (3)
- Fat Embolism SyndromeDocument26 pagesFat Embolism SyndromeAzni MokhtarPas encore d'évaluation
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Normal LabourDocument32 pagesNormal LabourUjjawalShriwastav100% (1)
- Abnormalities of PuerperiumDocument16 pagesAbnormalities of PuerperiumUjjawalShriwastavPas encore d'évaluation
- PneumoniaDocument63 pagesPneumoniaUjjawalShriwastavPas encore d'évaluation
- Metallic PoisonsDocument29 pagesMetallic PoisonsUjjawalShriwastavPas encore d'évaluation
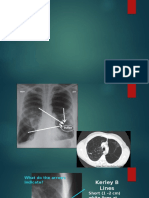
- Rad-Part 1Document21 pagesRad-Part 1UjjawalShriwastavPas encore d'évaluation
- Dr. Abhishek Karn Dept. of Forensic Medicine & ToxicologyDocument24 pagesDr. Abhishek Karn Dept. of Forensic Medicine & ToxicologyUjjawalShriwastavPas encore d'évaluation
- Nerve TraumaDocument31 pagesNerve TraumaUjjawalShriwastavPas encore d'évaluation
- ProteinuriasDocument32 pagesProteinuriasUjjawalShriwastavPas encore d'évaluation
- Rad Part 2Document21 pagesRad Part 2UjjawalShriwastavPas encore d'évaluation
- Cns StimulantsDocument37 pagesCns StimulantsUjjawalShriwastavPas encore d'évaluation
- IMCIintroduction For Medical StudentsDocument29 pagesIMCIintroduction For Medical StudentsUjjawalShriwastavPas encore d'évaluation
- Acute and Chronic PharyngitisDocument10 pagesAcute and Chronic PharyngitisUjjawalShriwastavPas encore d'évaluation
- FeverDocument26 pagesFeverUjjawalShriwastav100% (1)
- StarvationDocument23 pagesStarvationUjjawalShriwastav100% (1)
- Ilar Subtype Peak Age of Onset F: M Ratio % of All JIA Cases Arthritis Pattern Extra-Articular Features Lab Investigations Notes On TherapyDocument1 pageIlar Subtype Peak Age of Onset F: M Ratio % of All JIA Cases Arthritis Pattern Extra-Articular Features Lab Investigations Notes On TherapyUjjawalShriwastavPas encore d'évaluation
- Electrical InjuriesDocument26 pagesElectrical InjuriesUjjawalShriwastavPas encore d'évaluation
- Cardiac PoisonsDocument22 pagesCardiac PoisonsUjjawalShriwastavPas encore d'évaluation
- Fme Swot AnalysisDocument33 pagesFme Swot Analysismcad_mariePas encore d'évaluation
- Medicolegal Aspect of WoundDocument16 pagesMedicolegal Aspect of WoundUjjawalShriwastavPas encore d'évaluation
- Nepalese Legal ProvisionDocument32 pagesNepalese Legal ProvisionUjjawalShriwastavPas encore d'évaluation
- AudiometryDocument43 pagesAudiometryUjjawalShriwastavPas encore d'évaluation
- Benign Paroxysmal Positional Vertigo (BPPV)Document91 pagesBenign Paroxysmal Positional Vertigo (BPPV)UjjawalShriwastavPas encore d'évaluation
- UveitisDocument35 pagesUveitisUjjawalShriwastavPas encore d'évaluation
- KawasakiDocument20 pagesKawasakigail c dimacaliPas encore d'évaluation
- Roundworm (Ascaris Lumbricoides) : Morphology, Life Cycle & Laboratory DiagnosisDocument14 pagesRoundworm (Ascaris Lumbricoides) : Morphology, Life Cycle & Laboratory DiagnosisUjjawalShriwastavPas encore d'évaluation
- Facial Nerve Anatomy and Related PathologyDocument19 pagesFacial Nerve Anatomy and Related PathologyUjjawalShriwastavPas encore d'évaluation
- AdenoidsDocument8 pagesAdenoidsUjjawalShriwastavPas encore d'évaluation
- Tumori Tesuturi MoiDocument123 pagesTumori Tesuturi MoiOana BarbuPas encore d'évaluation
- Guidance For Industry Substantiation For Dietary Supplement Claims Made Under Section 403 (R) (6) of The Federal Food Drug and Cosmetic ActDocument18 pagesGuidance For Industry Substantiation For Dietary Supplement Claims Made Under Section 403 (R) (6) of The Federal Food Drug and Cosmetic ActDeepa PatelPas encore d'évaluation
- 11 Common Symptoms of CandidaDocument12 pages11 Common Symptoms of Candidasantana2013Pas encore d'évaluation
- Academy For Five Element Acupuncture Catalog 2013Document72 pagesAcademy For Five Element Acupuncture Catalog 2013Shari Blake40% (5)
- 2016 ACPL Expanded Content OutlineDocument9 pages2016 ACPL Expanded Content OutlineiisforintheskyPas encore d'évaluation
- Integrated Management of Childhood Illness (IMCI) : Printer-Friendly PDFDocument4 pagesIntegrated Management of Childhood Illness (IMCI) : Printer-Friendly PDFdaryl ann dep-asPas encore d'évaluation
- AclsDocument5 pagesAclsAnonymous vUl83IptiSPas encore d'évaluation
- Zoll M Series Defibrillator Manual PDFDocument111 pagesZoll M Series Defibrillator Manual PDFAhmad TanveerPas encore d'évaluation
- RA 7305 The Magna Carta of Public Health WorkersDocument11 pagesRA 7305 The Magna Carta of Public Health WorkersJessie Espino Vega100% (1)
- Argaud Et Al. - 2018 - Facial Emotion Recognition in Parkinson's Disease A Review and New HypothesesDocument14 pagesArgaud Et Al. - 2018 - Facial Emotion Recognition in Parkinson's Disease A Review and New HypothesesAleja ToPaPas encore d'évaluation
- Lithium Use in Pregnancy and The Risk of Cardiac MalformationsDocument10 pagesLithium Use in Pregnancy and The Risk of Cardiac MalformationsRoberto López MataPas encore d'évaluation
- Mode of Action of Functional Appliances / Orthodontic Courses by Indian Dental AcademyDocument116 pagesMode of Action of Functional Appliances / Orthodontic Courses by Indian Dental Academyindian dental academyPas encore d'évaluation
- Who Is Suitable For Cognitive Behavioural TherapyDocument8 pagesWho Is Suitable For Cognitive Behavioural TherapyPentheus214Pas encore d'évaluation
- Codeine Phosphate (Drug Study)Document2 pagesCodeine Phosphate (Drug Study)Franz.thenurse6888100% (2)
- Insomnia: Management of Underlying ProblemsDocument6 pagesInsomnia: Management of Underlying Problems7OrangesPas encore d'évaluation
- Erb's PalsyDocument18 pagesErb's PalsyMegha PataniPas encore d'évaluation
- Enema PresentationDocument34 pagesEnema PresentationVishalni Menon Returnz100% (2)
- CKD Pocket GuideDocument2 pagesCKD Pocket GuideLutfi MalefoPas encore d'évaluation
- Chapter 27 Chest InjuriesDocument70 pagesChapter 27 Chest Injuriesventus virPas encore d'évaluation
- Texas Has The Highest Maternal Mortality Rate in The Developed WorldDocument5 pagesTexas Has The Highest Maternal Mortality Rate in The Developed WorldDixanetPas encore d'évaluation
- Allergy Diagnosis Reference GuideDocument10 pagesAllergy Diagnosis Reference GuidevanjadamjanovicPas encore d'évaluation
- Arch-En-Design New Delhi / LucknowDocument12 pagesArch-En-Design New Delhi / LucknowMC EstimationPas encore d'évaluation
- Acute Kidney InjuryDocument8 pagesAcute Kidney InjuryAchmadNuryadiPas encore d'évaluation
- Narrative Report-Mam Monsanto2Document3 pagesNarrative Report-Mam Monsanto2Annie Lucrecia Mallari AguinaldoPas encore d'évaluation
- Adrenal Tumor-Pheochromocytoma 10-10-19Document30 pagesAdrenal Tumor-Pheochromocytoma 10-10-19JessicaPas encore d'évaluation
- DVT PreventionDocument8 pagesDVT PreventionRonald ThakorPas encore d'évaluation
- Anxiety Disorders in ChildrenDocument3 pagesAnxiety Disorders in ChildrenooiseowwweiPas encore d'évaluation