Vous aimerez peut-être aussi
- Acupressure Masterclass Treatment Chart ManualDocument114 pagesAcupressure Masterclass Treatment Chart ManualAkchika0% (2)
- Early Pregnancy Anomaly ScanDocument80 pagesEarly Pregnancy Anomaly ScanCezara Si Bogdan Muresan100% (3)
- Management of Tuberculosis: A guide for clinicians (eBook edition)D'EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Pas encore d'évaluation
- Thyroid StormDocument33 pagesThyroid StormVaibhav Krishna50% (2)
- Schizophrenia: Disturbances Thinking in Feeling BehaviorDocument26 pagesSchizophrenia: Disturbances Thinking in Feeling BehaviorVaibhav KrishnaPas encore d'évaluation
- Dissociation DisorderDocument33 pagesDissociation DisorderVaibhav KrishnaPas encore d'évaluation
- VSDDocument29 pagesVSDVaibhav Krishna100% (2)
- Neonatal JaundiceDocument33 pagesNeonatal JaundiceVaibhav Krishna100% (2)
- Maternal Child Tracking Sysem PDFDocument9 pagesMaternal Child Tracking Sysem PDFMegha MalhiPas encore d'évaluation
- History Taking in OrthopaedicsDocument23 pagesHistory Taking in OrthopaedicsVaibhav Krishna100% (5)
- Overview of India's Revised National Tuberculosis Control ProgrammeDocument65 pagesOverview of India's Revised National Tuberculosis Control Programmecatalyst1986100% (1)
- Subject: Obstetrical and Gynaecological Nursing: Submitted To: Mrs. Jyothi Prince Professor Apollo College of NursingDocument26 pagesSubject: Obstetrical and Gynaecological Nursing: Submitted To: Mrs. Jyothi Prince Professor Apollo College of NursingBeulah DasariPas encore d'évaluation
- Proplased Umbilical CordDocument2 pagesProplased Umbilical Cordkurlstein94% (17)
- HIV SeminarDocument20 pagesHIV SeminarRoselineTiggaPas encore d'évaluation
- Introduction To Pediatric NursingDocument36 pagesIntroduction To Pediatric Nursingcharan poonia100% (1)
- 3rd Stage of LabourDocument16 pages3rd Stage of LabourVaibhav KrishnaPas encore d'évaluation
- Shoulder DystociaDocument38 pagesShoulder DystociaVaibhav Krishna100% (1)
- MCHDocument5 pagesMCHNaiza Razul Makulit100% (3)
- Malnutrition in Indian ChildrenDocument29 pagesMalnutrition in Indian ChildrenDeep DavePas encore d'évaluation
- Maternal HealthDocument43 pagesMaternal HealthAsfand KhanPas encore d'évaluation
- National population policy goalsDocument23 pagesNational population policy goalssaarika_saini1017Pas encore d'évaluation
- Immunization Programme and Preventive Immunization: Presented By: Kanchan MSC 1 YRDocument53 pagesImmunization Programme and Preventive Immunization: Presented By: Kanchan MSC 1 YRArchanaPas encore d'évaluation
- Prevention of Parent To Child Transmission of HIV : Dr. ShobhaDocument52 pagesPrevention of Parent To Child Transmission of HIV : Dr. ShobhajijaniPas encore d'évaluation
- Fertilization, Implantation & Embryo Development ExplainedDocument54 pagesFertilization, Implantation & Embryo Development ExplainedMarvelousPas encore d'évaluation
- Worm Infestation in ChildrenDocument4 pagesWorm Infestation in ChildrenOleOhhPas encore d'évaluation
- Effectiveness of Video Assisted Teaching Module On Knowledge and Attitude Regarding Health Effects of Internet Addiction Disorders Among AdolescentsDocument4 pagesEffectiveness of Video Assisted Teaching Module On Knowledge and Attitude Regarding Health Effects of Internet Addiction Disorders Among AdolescentsAnonymous lAfk9gNPPas encore d'évaluation
- Mother and Child Protection Card: Paste Photo of Child HereDocument32 pagesMother and Child Protection Card: Paste Photo of Child HereMoham'medAlthafAs'lam100% (1)
- ScoringDocument53 pagesScoringKaran SinghPas encore d'évaluation
- Guidance & Counseling": Rajesh Kumar LecturerDocument19 pagesGuidance & Counseling": Rajesh Kumar LecturerLove DhaliwalPas encore d'évaluation
- IMNCIDocument19 pagesIMNCIdocsaurabh777Pas encore d'évaluation
- Nephrotic SyndromeeDocument28 pagesNephrotic SyndromeeRiteka SinghPas encore d'évaluation
- IPHS Fo SC PHC CHCDocument18 pagesIPHS Fo SC PHC CHCDrArun SinghPas encore d'évaluation
- Diabetes Mellitus in ChildrenDocument10 pagesDiabetes Mellitus in Childrenapi-322579342Pas encore d'évaluation
- IDD Control ProgrammeDocument13 pagesIDD Control ProgrammeathirabprasadPas encore d'évaluation
- Evaluation and Educational Programs in Nursing Course and Program NSG Education.Document10 pagesEvaluation and Educational Programs in Nursing Course and Program NSG Education.Akanksha NikunjPas encore d'évaluation
- Health Care Delivery System in India: Prepared by Aswani P Second Year MSC Nursing Govt. College of NursingDocument88 pagesHealth Care Delivery System in India: Prepared by Aswani P Second Year MSC Nursing Govt. College of Nursingprabha krishnanPas encore d'évaluation
- Updated Operational Guidelines For Mission IndradhanushDocument76 pagesUpdated Operational Guidelines For Mission IndradhanushZLOOffice BankuraPas encore d'évaluation
- National Nutrition Programm and PolicyDocument15 pagesNational Nutrition Programm and PolicyDr.ekta singh chauhan100% (1)
- Imnci PPT KapilDocument65 pagesImnci PPT KapilkapilPas encore d'évaluation
- Anti Malaria PPT SajidDocument18 pagesAnti Malaria PPT SajidAaban AdilaPas encore d'évaluation
- Nursing Care of Disable PeopleDocument40 pagesNursing Care of Disable PeoplePraZeeTaPuriPas encore d'évaluation
- Organic Brain DisorderDocument69 pagesOrganic Brain DisorderHowell Mathew100% (1)
- CURRENT STATUS-WPS OfficeDocument35 pagesCURRENT STATUS-WPS OfficeVinnyPas encore d'évaluation
- NEONATAL INFECTIONS: CAUSES, SIGNS AND TREATMENTDocument86 pagesNEONATAL INFECTIONS: CAUSES, SIGNS AND TREATMENTSanjay Kumar SanjuPas encore d'évaluation
- Factors Influencing LearningDocument17 pagesFactors Influencing Learningnirajan shresthaPas encore d'évaluation
- Teachers Role in Managing Non Projected ADocument23 pagesTeachers Role in Managing Non Projected Amanju meenaPas encore d'évaluation
- National AIDS Control Programme Phase-IV: Current Status and Critical AppraisalDocument71 pagesNational AIDS Control Programme Phase-IV: Current Status and Critical AppraisalNeethu Vincent100% (1)
- Hirschsprung'S Disease (Megacolon) : Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkaraDocument6 pagesHirschsprung'S Disease (Megacolon) : Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkarakrishnasreePas encore d'évaluation
- Major stakeholders in the healthcare system government, providers, publicDocument2 pagesMajor stakeholders in the healthcare system government, providers, publicShilpi SinghPas encore d'évaluation
- National health programmes overviewDocument40 pagesNational health programmes overviewGaoudam NatarajanPas encore d'évaluation
- Bonding NewDocument23 pagesBonding NewPadmaPas encore d'évaluation
- Iec AnpDocument16 pagesIec AnpValarmathiPas encore d'évaluation
- Health Care Delivery SystemDocument75 pagesHealth Care Delivery SystemSudha YadavPas encore d'évaluation
- Nursing Care PneumoniaDocument26 pagesNursing Care PneumoniaIsaac Kipkemoi100% (1)
- Ppt-Journal ClubDocument50 pagesPpt-Journal Clubgao1989Pas encore d'évaluation
- ICDS Scheme ExplainedDocument59 pagesICDS Scheme ExplainedRamniwasMahorePas encore d'évaluation
- The Joint Committee On Health Education and Promotion Terminology of 2001 Defined Health Education As "AnyDocument8 pagesThe Joint Committee On Health Education and Promotion Terminology of 2001 Defined Health Education As "AnyRaman SamraoPas encore d'évaluation
- Refractive ErrorDocument6 pagesRefractive Errortri erdiansyahPas encore d'évaluation
- M.sc. Nursing Syllabus 0108Document142 pagesM.sc. Nursing Syllabus 0108Nikhil DahiyaPas encore d'évaluation
- Tele-Medicine and Tele - Nursing Kathing2Document33 pagesTele-Medicine and Tele - Nursing Kathing2kathing gatinPas encore d'évaluation
- Seminar 2 Endocrine DisordersDocument44 pagesSeminar 2 Endocrine DisordersSuganthi ParthibanPas encore d'évaluation
- Health Insurance SchemeDocument10 pagesHealth Insurance SchemeKailash NagarPas encore d'évaluation
- FAMILY CARE STUDY (FORMATDocument13 pagesFAMILY CARE STUDY (FORMATLavanya ChPas encore d'évaluation
- Safemotherhood 130212085105 Phpapp01Document32 pagesSafemotherhood 130212085105 Phpapp01daniel laoatenPas encore d'évaluation
- Advanced Nursing Practice: M.Sc. Degree Course in NursingDocument58 pagesAdvanced Nursing Practice: M.Sc. Degree Course in NursingEsha KuttiPas encore d'évaluation
- National Health Programmes For Children in IndiaDocument79 pagesNational Health Programmes For Children in IndiashahnazPas encore d'évaluation
- Legal Aspects and EthicsDocument18 pagesLegal Aspects and EthicsBuyung Tegar AribowoPas encore d'évaluation
- Failure to Thrive TeachingDocument10 pagesFailure to Thrive TeachingSAYMABANUPas encore d'évaluation
- Treatment Aspects in Perioperative NursingDocument51 pagesTreatment Aspects in Perioperative NursingShibin Jacob100% (2)
- National Leprosy Eradication Program (Nlep: Dr. Kanupriya ChaturvediDocument24 pagesNational Leprosy Eradication Program (Nlep: Dr. Kanupriya ChaturvediLavendra KunwarPas encore d'évaluation
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesD'EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesPas encore d'évaluation
- VITILIGODocument21 pagesVITILIGOVaibhav KrishnaPas encore d'évaluation
- Manipal College of Medical Sciences Pokhara, Nepal: Erythema MultiformeDocument56 pagesManipal College of Medical Sciences Pokhara, Nepal: Erythema MultiformeVaibhav KrishnaPas encore d'évaluation
- Acute Leukaemia Presentation 1Document20 pagesAcute Leukaemia Presentation 1Vaibhav KrishnaPas encore d'évaluation
- Specific Types of DysnpeaDocument14 pagesSpecific Types of DysnpeaPiyush Agarwal100% (1)
- Approach To AnemiaDocument33 pagesApproach To AnemiaVaibhav KrishnaPas encore d'évaluation
- UTI Tubulointerstitial DrugsDocument43 pagesUTI Tubulointerstitial DrugsVaibhav KrishnaPas encore d'évaluation
- Acute Leukaemia Presentation 1Document20 pagesAcute Leukaemia Presentation 1Vaibhav KrishnaPas encore d'évaluation
- Kernicterus: Sahisnuta BasnetDocument10 pagesKernicterus: Sahisnuta BasnetVaibhav KrishnaPas encore d'évaluation
- Chest PainDocument23 pagesChest PainVaibhav KrishnaPas encore d'évaluation
- Anxiety DisorderDocument26 pagesAnxiety DisorderVaibhav KrishnaPas encore d'évaluation
- LEUKEMIAsDocument56 pagesLEUKEMIAsVaibhav KrishnaPas encore d'évaluation
- Abdominal Pain in ChildrenDocument15 pagesAbdominal Pain in ChildrenVaibhav KrishnaPas encore d'évaluation
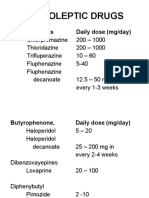
- Neuroleptic Drugs: Phenothiazines Daily Dose (Mg/day)Document11 pagesNeuroleptic Drugs: Phenothiazines Daily Dose (Mg/day)Vaibhav KrishnaPas encore d'évaluation
- Antidepressants: I. Cyclic AntidepressantDocument17 pagesAntidepressants: I. Cyclic AntidepressantVaibhav KrishnaPas encore d'évaluation
- Prenatal Teaching PlanDocument3 pagesPrenatal Teaching PlanᅮᅮAmalPas encore d'évaluation
- Endocrine System in FinfishesDocument43 pagesEndocrine System in FinfishesMisbah SayyedPas encore d'évaluation
- Ethical Issues in Assisted Reproductive Technologies ART 2Document49 pagesEthical Issues in Assisted Reproductive Technologies ART 2Pavan chowdaryPas encore d'évaluation
- Quarter3 Week 1: (MELC) : Compose An Argumentative Essay Reference: English 10 Learner's Material - Celebrating DiversityDocument7 pagesQuarter3 Week 1: (MELC) : Compose An Argumentative Essay Reference: English 10 Learner's Material - Celebrating Diversitymy musicPas encore d'évaluation
- Breast Development and Morphology - UpToDateDocument43 pagesBreast Development and Morphology - UpToDateAndrea Díaz Rodríguez0% (1)
- Newborn Movement Assessment 1687969489Document68 pagesNewborn Movement Assessment 1687969489Selva Srinivasan mPas encore d'évaluation
- Nursing Simulation - Patient EvaluationDocument3 pagesNursing Simulation - Patient EvaluationAaronPas encore d'évaluation
- Placenta PreviaDocument5 pagesPlacenta PreviaKuro HanabusaPas encore d'évaluation
- Physiology of The Reproductive For Nursing To Be PresentDocument96 pagesPhysiology of The Reproductive For Nursing To Be PresentraphatoelPas encore d'évaluation
- Menstrual Disorders - SDYV TTC-2Document86 pagesMenstrual Disorders - SDYV TTC-2Joanna EvansPas encore d'évaluation
- Group - 4 Final ManuscriptDocument137 pagesGroup - 4 Final ManuscriptNoah Jared MasangkayPas encore d'évaluation
- 1696-Article Text-4009-1-10-20201129Document5 pages1696-Article Text-4009-1-10-20201129asmita sainiPas encore d'évaluation
- 6 Minute English Food For New MumsDocument5 pages6 Minute English Food For New MumsWilliamMonteroRomeroPas encore d'évaluation
- NCM 107 Skills LaboratoryDocument27 pagesNCM 107 Skills LaboratoryCharlmagne LinnamPas encore d'évaluation
- Sexual Disorders GuideDocument60 pagesSexual Disorders GuideRakesh KumarPas encore d'évaluation
- 5663 PDFDocument7 pages5663 PDFwaelPas encore d'évaluation
- Relationship between accuracy of main diagnosis medical terminology and coding accuracyDocument10 pagesRelationship between accuracy of main diagnosis medical terminology and coding accuracyPutri Aisya MaulidaPas encore d'évaluation
- Isuog: GuidelinesDocument17 pagesIsuog: GuidelinesAndrés Gaviria CPas encore d'évaluation
- Chapter IDocument7 pagesChapter IRenze Meinard MortigaPas encore d'évaluation
- 11 Benefits of Breastfeeding For Both Mom and BabyDocument14 pages11 Benefits of Breastfeeding For Both Mom and BabyMac Cristian A. CaraganPas encore d'évaluation
- The Menstrual Cycle Learning Activity SheetDocument4 pagesThe Menstrual Cycle Learning Activity SheetTampok ES (Region III - Bulacan)Pas encore d'évaluation
- Lesson 05. Mammary GlandsDocument23 pagesLesson 05. Mammary GlandsLola PPas encore d'évaluation
- METHODDocument13 pagesMETHODGwagsiGlennPas encore d'évaluation
- Condom FemaleDocument7 pagesCondom FemaleHuyền ÁnhPas encore d'évaluation
- Multilevel Survival Analysis of Factors Associated.13Document8 pagesMultilevel Survival Analysis of Factors Associated.13ShaileshPas encore d'évaluation
- Reproduction and Development Study GuideDocument9 pagesReproduction and Development Study GuidemattvprPas encore d'évaluation
- Synopsis For Registration of Title of Thesis For M.D. (Community Medicine)Document14 pagesSynopsis For Registration of Title of Thesis For M.D. (Community Medicine)RamniwasMahorePas encore d'évaluation