Vous aimerez peut-être aussi
- Marasmus - Case ReportDocument13 pagesMarasmus - Case ReportApriany Cordias Arlita SilalahiPas encore d'évaluation
- Marasmus and Kwashiokor - Dr. YaranDocument23 pagesMarasmus and Kwashiokor - Dr. YaranBashar KhalilPas encore d'évaluation
- PPP - Kwashiorkor & MarasmusDocument19 pagesPPP - Kwashiorkor & MarasmusJanine Kristine ManaoisPas encore d'évaluation
- I. Severe Protein-Energy Malnutrition (PEM) : A. General Considerations On PEMDocument6 pagesI. Severe Protein-Energy Malnutrition (PEM) : A. General Considerations On PEMReg LagartejaPas encore d'évaluation
- SGD 4 - Skeletal Muscle PhysiologyDocument3 pagesSGD 4 - Skeletal Muscle PhysiologyKriska Noelle0% (1)
- Pku AlkDocument33 pagesPku AlkSharf WangPas encore d'évaluation
- KwashiorkorDocument4 pagesKwashiorkorreshma banuPas encore d'évaluation
- NSAIDDocument15 pagesNSAIDMaria KhawajaPas encore d'évaluation
- Case Report: Kwashiorkor: BY: JAYA DEV (110100465) Supervisor: Dr. Hj. Tiangsa Sembiring, M.Ked (Ped), Sp.A (K)Document49 pagesCase Report: Kwashiorkor: BY: JAYA DEV (110100465) Supervisor: Dr. Hj. Tiangsa Sembiring, M.Ked (Ped), Sp.A (K)Izaac JdevPas encore d'évaluation
- Physiology Lab InstrumentsDocument9 pagesPhysiology Lab InstrumentsPhysiology by Dr Raghuveer100% (3)
- Nutritional Deficiency Disorder/ (PEM)Document37 pagesNutritional Deficiency Disorder/ (PEM)ShrutiPas encore d'évaluation
- Sample PrognosisDocument3 pagesSample PrognosisjudssalangsangPas encore d'évaluation
- Human Reflex PhysiologyDocument14 pagesHuman Reflex PhysiologyIhsanyPrihadi100% (1)
- Thalamus and HypothalamusDocument19 pagesThalamus and Hypothalamusapi-266034924Pas encore d'évaluation
- Attributes of The Learner Chapter 8Document31 pagesAttributes of The Learner Chapter 8Allyssa Lorraine Prudencio100% (1)
- (Biochem A) 1.3 Protein Chemistry (Santos)Document16 pages(Biochem A) 1.3 Protein Chemistry (Santos)JesziePas encore d'évaluation
- Lesson 1 Intro To BiochemDocument15 pagesLesson 1 Intro To BiochemJulius Memeg PanayoPas encore d'évaluation
- Clinical Presentation and Diagnosis of Tuberculosis: International Standards 1-5Document51 pagesClinical Presentation and Diagnosis of Tuberculosis: International Standards 1-5Gilbert Solomon TantonoPas encore d'évaluation
- Galactosemia by Group 9Document41 pagesGalactosemia by Group 9Sree Balaji Srinivas Katakam100% (1)
- Anaphy 100 Lab Practice Review Sheet 1 and 2Document6 pagesAnaphy 100 Lab Practice Review Sheet 1 and 2Mariam GamosPas encore d'évaluation
- Global Developmental DelayDocument2 pagesGlobal Developmental DelayAtlerPas encore d'évaluation
- Kwashiorkor 2Document13 pagesKwashiorkor 2Mutiara Riahna SitepuPas encore d'évaluation
- Activity No. 4 Amanda's Eating Habits: A Case Study: INSTRUCTION: Answer What Is Being Asked ForDocument4 pagesActivity No. 4 Amanda's Eating Habits: A Case Study: INSTRUCTION: Answer What Is Being Asked ForKarl Michael Cabañog50% (2)
- Metabolic AlkalosisDocument9 pagesMetabolic AlkalosisMohammad Zaki BudimanPas encore d'évaluation
- Anatomy and PhysiologyDocument11 pagesAnatomy and PhysiologyFiona Aaronica Hope LibrandaPas encore d'évaluation
- 05 - Sle, DMZ, PHSDocument157 pages05 - Sle, DMZ, PHSG SPas encore d'évaluation
- 1.introduction To BiochemistryDocument23 pages1.introduction To BiochemistryIslam SamirPas encore d'évaluation
- Fatty Acid Oxidation & Ketone BodiesDocument30 pagesFatty Acid Oxidation & Ketone BodiesM.PRASAD NAIDUPas encore d'évaluation
- Glycogen Storage Disorders PDFDocument4 pagesGlycogen Storage Disorders PDFAHMEDPas encore d'évaluation
- Kay - OR CaseDocument9 pagesKay - OR CaseSienaPas encore d'évaluation
- Multiple SclerosisDocument6 pagesMultiple SclerosisandrearuzziPas encore d'évaluation
- GALACTOSEMIAlabDocument49 pagesGALACTOSEMIAlabShen VillamilPas encore d'évaluation
- Phenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeDocument24 pagesPhenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeAsfoor gake1Pas encore d'évaluation
- Impact of Globalization On Pakistan111Document12 pagesImpact of Globalization On Pakistan111Sheraz AliPas encore d'évaluation
- 3LP 2020ncm105Document7 pages3LP 2020ncm105Margarette GeresPas encore d'évaluation
- Nursing Care of at RiskDocument7 pagesNursing Care of at RiskdominicjimenezPas encore d'évaluation
- Case StudyDocument4 pagesCase StudyAngela Mae DimayacyacPas encore d'évaluation
- 1Document13 pages1Anonymous XfdS5dDPas encore d'évaluation
- Protein MetabolismDocument15 pagesProtein MetabolismAfshan Akhtar100% (1)
- Hormone Feedback LoopsDocument6 pagesHormone Feedback LoopsSylheti BabaPas encore d'évaluation
- Lec 1 Enzyme and Its ClassificationDocument30 pagesLec 1 Enzyme and Its ClassificationSadia DinPas encore d'évaluation
- DYSTROPHYDocument15 pagesDYSTROPHYleeyan2wenty6Pas encore d'évaluation
- Health Assessment: An: Diana Rose D. Emerenciana, RN., ManDocument72 pagesHealth Assessment: An: Diana Rose D. Emerenciana, RN., ManSM CervantesPas encore d'évaluation
- ..Digestion of ProteinDocument21 pages..Digestion of Proteinaneeda shabirPas encore d'évaluation
- Cell Injury Pathology Chapter 01 NotesDocument6 pagesCell Injury Pathology Chapter 01 NotesAmeerHamzaPas encore d'évaluation
- Surgery - Care of Casts and TractionsDocument7 pagesSurgery - Care of Casts and TractionsMaria Eleni ÖPas encore d'évaluation
- Exercise Variables and PrinciplesDocument27 pagesExercise Variables and Principlesroselhyn SottoPas encore d'évaluation
- Acute GlomerulonephritisDocument27 pagesAcute GlomerulonephritisKumara GuruPas encore d'évaluation
- Session 1: Life Cycle and Goal Setting: Our Lady of Fatima University Veritas Et MisericordiaDocument6 pagesSession 1: Life Cycle and Goal Setting: Our Lady of Fatima University Veritas Et MisericordiaKylie Grace WiscoPas encore d'évaluation
- LAS 1-5 Answer KeysDocument12 pagesLAS 1-5 Answer KeysAlthea Joy Sincero BiocoPas encore d'évaluation
- Pig Heart Dissection Lab - Final PDFDocument15 pagesPig Heart Dissection Lab - Final PDFapi-1127245210% (1)
- Chronic Kidney DiseaseDocument13 pagesChronic Kidney DiseaseJobelle AcenaPas encore d'évaluation
- Bukidnon State UniversityDocument106 pagesBukidnon State UniversityfLOR_ZIANE_MAEPas encore d'évaluation
- THE LEVEL OF AWARENESS AMONG THE TEENAGE MOTHERS OF TUBIGON, BOHOL IN RENDERING NEWBORN CARE (Part 1)Document13 pagesTHE LEVEL OF AWARENESS AMONG THE TEENAGE MOTHERS OF TUBIGON, BOHOL IN RENDERING NEWBORN CARE (Part 1)Wuawie MemesPas encore d'évaluation
- Diabetes Mellitus: A Common Disease: EpidemiologyDocument4 pagesDiabetes Mellitus: A Common Disease: EpidemiologyPaul Kerbie Mateo ArrojoPas encore d'évaluation
- Glasgow Coma Scale: - Eye-Opening - Motor - Verbal ResponsesDocument13 pagesGlasgow Coma Scale: - Eye-Opening - Motor - Verbal ResponsesSofianPas encore d'évaluation
- Carbohydrate Metabolism .NursingEdutechDocument90 pagesCarbohydrate Metabolism .NursingEdutechjmbrand jmPas encore d'évaluation
- Neurological Assessment (Adult) : Group 4Document99 pagesNeurological Assessment (Adult) : Group 4Marriam LegazpiPas encore d'évaluation
- PrenatalDocument1 pagePrenatalJohn Patrick G. GuevarraPas encore d'évaluation
- Marasmus and KwashiorkorDocument52 pagesMarasmus and KwashiorkorMelissa Salayog100% (4)
- Fig.1: Vegetative Morphology of EctocarpusDocument21 pagesFig.1: Vegetative Morphology of EctocarpusAmrit Mund EducationalPas encore d'évaluation
- 7 week:: Microbial Growth (미생물의 성장)Document24 pages7 week:: Microbial Growth (미생물의 성장)MoonHoLeePas encore d'évaluation
- Cold Spring Harb Perspect Med-2017-Long-a025577 PDFDocument17 pagesCold Spring Harb Perspect Med-2017-Long-a025577 PDFAurelia WetondiePas encore d'évaluation
- NeoplasiaDocument21 pagesNeoplasiaFreakyRustlee LeoragPas encore d'évaluation
- Markscheme HL Paper3Document8 pagesMarkscheme HL Paper3Jane ChangPas encore d'évaluation
- Keragaman Jeruk Fungsional Indonesia Berdasarkan Karakter Morfologis Dan Marka RAPDDocument10 pagesKeragaman Jeruk Fungsional Indonesia Berdasarkan Karakter Morfologis Dan Marka RAPDUlfahPas encore d'évaluation
- DNA Sequencing by Capillary Electrophoresis Chemistry GuideDocument310 pagesDNA Sequencing by Capillary Electrophoresis Chemistry GuidepicapenasPas encore d'évaluation
- BioinformaticsDocument167 pagesBioinformaticsGilbert MethewPas encore d'évaluation
- שיטות מעבדה ביולוגיה מולקולריתDocument53 pagesשיטות מעבדה ביולוגיה מולקולריתKamal KabhaPas encore d'évaluation
- Discuss Genetic Factors in AggressionDocument2 pagesDiscuss Genetic Factors in AggressionmopheadfattyPas encore d'évaluation
- AnaPhy - Digestive SystemDocument11 pagesAnaPhy - Digestive SystemGia P. de VeyraPas encore d'évaluation
- Pharmaceutical BotanyDocument10 pagesPharmaceutical BotanyJan Chrispian MirasolPas encore d'évaluation
- Passive and Active Transport Internet AssignmentDocument4 pagesPassive and Active Transport Internet AssignmentShalu PundirPas encore d'évaluation
- Superoxide Dismutase (SOD) A Promising Enzyme in The Area of Biopharmaceuticals in Its Native and Immobilized Form A ReviewDocument9 pagesSuperoxide Dismutase (SOD) A Promising Enzyme in The Area of Biopharmaceuticals in Its Native and Immobilized Form A ReviewIJRASETPublicationsPas encore d'évaluation
- Digestion and Absorption 111Document6 pagesDigestion and Absorption 111Brijesh BalachandranPas encore d'évaluation
- Transgene: Transparent FrogDocument3 pagesTransgene: Transparent Froggeobee emmanuelPas encore d'évaluation
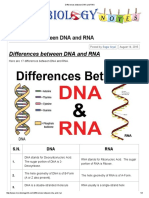
- Differences Between DNA and RNADocument3 pagesDifferences Between DNA and RNAMeri SunderPas encore d'évaluation
- Drosophilia Lab ReportDocument5 pagesDrosophilia Lab ReportMaddie BleasePas encore d'évaluation
- Science August 14 2009Document95 pagesScience August 14 2009Greg_G100% (1)
- Genetic Linkage, Recombination, Mapping - BIO231-FKDocument9 pagesGenetic Linkage, Recombination, Mapping - BIO231-FKmalik husnainPas encore d'évaluation
- Haemogram: Blood CountsDocument3 pagesHaemogram: Blood CountsAbhi PrajapatiPas encore d'évaluation
- Historyof Genetics QuizDocument2 pagesHistoryof Genetics QuizGelli NancaPas encore d'évaluation
- Tips For BiologyDocument15 pagesTips For BiologyMasega Daniel ManaliPas encore d'évaluation
- Chapter21 PDFDocument25 pagesChapter21 PDFsgw67Pas encore d'évaluation
- Biodiversity and Ecosystem ServicesDocument18 pagesBiodiversity and Ecosystem Servicessameer AhadPas encore d'évaluation
- Compost Tea Brewing ManualDocument91 pagesCompost Tea Brewing ManualJanetS14338100% (1)
- November 2006 MS - Paper 3 CIE Biology IGCSEDocument6 pagesNovember 2006 MS - Paper 3 CIE Biology IGCSEUzair ZahidPas encore d'évaluation
- Real Time PCR: Pramod Bahadur K.CDocument14 pagesReal Time PCR: Pramod Bahadur K.CPramod KcPas encore d'évaluation
- Dermo Disease of OysterDocument4 pagesDermo Disease of OysterSophia ManzanoPas encore d'évaluation
- Natural Antimicrobial and Bioactive Compounds From Ludwigia Parviflora RoxbDocument6 pagesNatural Antimicrobial and Bioactive Compounds From Ludwigia Parviflora Roxbnguyen ba trungPas encore d'évaluation