Vous aimerez peut-être aussi
- Competence Appraisal Cesarean SectionDocument20 pagesCompetence Appraisal Cesarean SectionAnaPas encore d'évaluation
- The IntegumentDocument1 pageThe IntegumentAnaPas encore d'évaluation
- The IntegumentDocument17 pagesThe IntegumentAnaPas encore d'évaluation
- Abnormal Progress in Labor (Precipitous Labor and Birth & Retraction Rings)Document34 pagesAbnormal Progress in Labor (Precipitous Labor and Birth & Retraction Rings)Ana100% (3)
- Beliefs and Material Culture in The PhilippinesDocument4 pagesBeliefs and Material Culture in The PhilippinesAnaPas encore d'évaluation
- Competence Appraisal Cesarean SectionDocument20 pagesCompetence Appraisal Cesarean SectionAnaPas encore d'évaluation
- Soc Sci ReportDocument69 pagesSoc Sci ReportAnaPas encore d'évaluation
- Placenta Accreta ReportDocument13 pagesPlacenta Accreta ReportAnaPas encore d'évaluation
- A Case Study On Typhoid FeverDocument42 pagesA Case Study On Typhoid FeverAna92% (13)
- Chest PhysiotherapyDocument5 pagesChest PhysiotherapyAnaPas encore d'évaluation
- Soapie, Assessment and NCP On PAINDocument7 pagesSoapie, Assessment and NCP On PAINAna100% (2)
- Uterine AnomaliesDocument24 pagesUterine AnomaliesAnaPas encore d'évaluation
- FNCPDocument9 pagesFNCPAna100% (4)
- Retraction RingDocument5 pagesRetraction RingAna100% (2)
- Retraction Ring LeafletDocument2 pagesRetraction Ring LeafletAna100% (1)
- Immune SystemDocument58 pagesImmune SystemAnaPas encore d'évaluation
- Different Substance Abuse and Their Effects To Pregnancy and FetusDocument5 pagesDifferent Substance Abuse and Their Effects To Pregnancy and FetusAnaPas encore d'évaluation
- DM-Health Teaching PlanDocument9 pagesDM-Health Teaching PlanAna86% (7)
- Prokaryotic & Eukaryotic Cells - 3Document47 pagesProkaryotic & Eukaryotic Cells - 3AnaPas encore d'évaluation
- Assignment in NutritionDocument12 pagesAssignment in NutritionAnaPas encore d'évaluation
- Immunization SchedulesDocument3 pagesImmunization SchedulesAnaPas encore d'évaluation
- CVA-Health Teaching PlanDocument5 pagesCVA-Health Teaching PlanAna100% (4)
- Immune System 2Document39 pagesImmune System 2AnaPas encore d'évaluation
- Nursery Rhyme ActivitiesDocument13 pagesNursery Rhyme ActivitiesAnaPas encore d'évaluation
- Stroke (Bisaya and English)Document4 pagesStroke (Bisaya and English)AnaPas encore d'évaluation
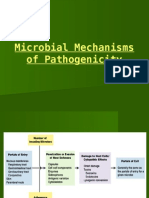
- Microbial Mechanisms of PathogenicityDocument29 pagesMicrobial Mechanisms of PathogenicityAnaPas encore d'évaluation
- SporotrichosisDocument5 pagesSporotrichosisAna100% (1)
- Microbial Diseases of The Skin & EyesDocument52 pagesMicrobial Diseases of The Skin & EyesAna100% (3)
- Microbial Diseases of The Respiratory SystemDocument9 pagesMicrobial Diseases of The Respiratory SystemAnaPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Elements (Industrial Plant)Document5 pagesElements (Industrial Plant)Veralyn Mae BondadPas encore d'évaluation
- Agemp Two MarksDocument8 pagesAgemp Two MarksKishore CrazePas encore d'évaluation
- Commercial Inverter AC Service ManualDocument116 pagesCommercial Inverter AC Service ManualEdwin JaramilloPas encore d'évaluation
- 1 s2.0 S2667345222000104 MainDocument19 pages1 s2.0 S2667345222000104 MainJosiah MwashitaPas encore d'évaluation
- Govt Schemes - 1 MWCD MOSJEDocument36 pagesGovt Schemes - 1 MWCD MOSJEshaheen razaPas encore d'évaluation
- E IA Diagnostic Atmos Cube 2012-07-04Document32 pagesE IA Diagnostic Atmos Cube 2012-07-04RogerPas encore d'évaluation
- Lab Report 1Document3 pagesLab Report 1CarlEspantoPas encore d'évaluation
- Kovach 1987Document10 pagesKovach 1987Quyen ta thi nhaPas encore d'évaluation
- NCPDocument18 pagesNCPChristian Karl B. LlanesPas encore d'évaluation
- 700 - 900 Error Codes PDFDocument1 page700 - 900 Error Codes PDFIsai Lara OsoriaPas encore d'évaluation
- Cape Vincent Area Events January 2019Document5 pagesCape Vincent Area Events January 2019NewzjunkyPas encore d'évaluation
- Msae Msae2018-Arwm012 Full Dronespraying 2Document4 pagesMsae Msae2018-Arwm012 Full Dronespraying 2Muhammad Huzaifah Mohd RoslimPas encore d'évaluation
- Specifications of TES-593Document2 pagesSpecifications of TES-593symasiPas encore d'évaluation
- TVL ICT IllustrationNCII Q1Module2Document12 pagesTVL ICT IllustrationNCII Q1Module2Kimberly Trocio Kim100% (1)
- SF 9 - ES Learners Progress Report CardDocument3 pagesSF 9 - ES Learners Progress Report Cardroxanne50% (2)
- Understanding Steam Turbine VibrationDocument30 pagesUnderstanding Steam Turbine VibrationkatibraPas encore d'évaluation
- Geoheritage of Labuan Island: Bulletin of The Geological Society of Malaysia December 2016Document14 pagesGeoheritage of Labuan Island: Bulletin of The Geological Society of Malaysia December 2016songkkPas encore d'évaluation
- Everything You Need to Know About Gas Metal Arc Welding (GMAWDocument31 pagesEverything You Need to Know About Gas Metal Arc Welding (GMAWAhmetDuranCeyhanPas encore d'évaluation
- Traceability Summary - Supplies July 2015 - June 2016: PT Multimas Nabati Asahan, Kuala TanjungDocument4 pagesTraceability Summary - Supplies July 2015 - June 2016: PT Multimas Nabati Asahan, Kuala TanjungAbu KhalidPas encore d'évaluation
- New Accreditation ToolsDocument52 pagesNew Accreditation ToolsLyle Guion Paguio100% (1)
- LESSON 1 PREPARE VEGETABLE DISHES OverviDocument12 pagesLESSON 1 PREPARE VEGETABLE DISHES OverviKeym Garcia Galvez IIIPas encore d'évaluation
- 1 s2.0 S0149763418301957 MainDocument24 pages1 s2.0 S0149763418301957 MainjackPas encore d'évaluation
- Making your own Agar PlateDocument8 pagesMaking your own Agar PlateCheska EngadaPas encore d'évaluation
- EDC MS 6.4 System DescriptionDocument10 pagesEDC MS 6.4 System Descriptionmarsh2002Pas encore d'évaluation
- Corrosion and Its Objective QuestionsDocument2 pagesCorrosion and Its Objective QuestionsSrinivasan Alagappan100% (4)
- Round Warre HivesDocument16 pagesRound Warre HivesBender Rodríguez100% (1)
- AssignmentDocument2 pagesAssignmenttayyabauzairPas encore d'évaluation
- Home Study Report of Resident Indian Parent: Name of The Social WorkerDocument4 pagesHome Study Report of Resident Indian Parent: Name of The Social WorkerVmksPas encore d'évaluation
- Work Procedure For CCB Installation of Raised Floor 2Document13 pagesWork Procedure For CCB Installation of Raised Floor 2ResearcherPas encore d'évaluation
- Defined Contribution PlanDocument12 pagesDefined Contribution Planrap rapadasPas encore d'évaluation