Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
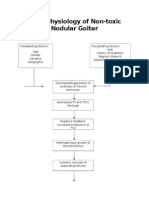
- Pathophysiology of Nontoxic Nodular GoiterDocument2 pagesPathophysiology of Nontoxic Nodular GoiterJan Jewey80% (10)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Cardiovascular & Respiratory System Immunology - PPT (Compatibility Mode)Document64 pagesCardiovascular & Respiratory System Immunology - PPT (Compatibility Mode)Mwanja MosesPas encore d'évaluation
- LampiranDocument9 pagesLampiranhara kurnia bPas encore d'évaluation
- Urolithiasis and Its Causes-Short Review: T. Vijaya, M. Sathish Kumar, N. V. Ramarao, A. Naredra Babu, N. RamaraoDocument6 pagesUrolithiasis and Its Causes-Short Review: T. Vijaya, M. Sathish Kumar, N. V. Ramarao, A. Naredra Babu, N. RamaraoLea Bali Ulina SinurayaPas encore d'évaluation
- Salinan Hasil Olda 1. Identitas Responden: StatisticsDocument5 pagesSalinan Hasil Olda 1. Identitas Responden: Statisticshara kurnia bPas encore d'évaluation
- Tugas Jurnal Reading Ikk PDFDocument11 pagesTugas Jurnal Reading Ikk PDFhara kurnia bPas encore d'évaluation
- Analisis PICO No. Question Components Your Question P - Patient or PopulationDocument1 pageAnalisis PICO No. Question Components Your Question P - Patient or Populationhara kurnia bPas encore d'évaluation
- Epi LepsiDocument1 pageEpi Lepsihara kurnia bPas encore d'évaluation
- EpilepsiDocument1 pageEpilepsihara kurnia bPas encore d'évaluation
- Medical Neuroscience Tutorial Notes: Overview of Neural SignalingDocument2 pagesMedical Neuroscience Tutorial Notes: Overview of Neural SignalingOmar AlemánPas encore d'évaluation
- Insuficiencia Renal CronicaDocument13 pagesInsuficiencia Renal CronicaCarlos DPas encore d'évaluation
- 12 Pairs of Cranial Nerves and Their FunctionsDocument37 pages12 Pairs of Cranial Nerves and Their FunctionsCiprian RataPas encore d'évaluation
- 606mv Could I Be A Living Kidney Donor Olc2064 Web 1Document16 pages606mv Could I Be A Living Kidney Donor Olc2064 Web 1Siti RahmawatiPas encore d'évaluation
- Neurophysiology Systems of the Brain and Spinal CordDocument50 pagesNeurophysiology Systems of the Brain and Spinal CordHomeground entertainmentPas encore d'évaluation
- Diarrhea Crampy Abdominal Pain Nausea OmitingDocument14 pagesDiarrhea Crampy Abdominal Pain Nausea OmitingLynne CammayoPas encore d'évaluation
- Physioloical Integrity Acute Biologic CrisisDocument42 pagesPhysioloical Integrity Acute Biologic CrisisJohn Paul M. TagapanPas encore d'évaluation
- ACCP Farmakoterapi 2013Document296 pagesACCP Farmakoterapi 2013Decy RahmawatiPas encore d'évaluation
- Met Caz ClinicDocument57 pagesMet Caz ClinicIndrecan AndreiPas encore d'évaluation
- Physiological Changes During PregnancyDocument44 pagesPhysiological Changes During PregnancyvrutipatelPas encore d'évaluation
- Strength endurance capabilitiesDocument1 pageStrength endurance capabilitiesWhooper GamestorPas encore d'évaluation
- Increased Intracranial PressureDocument2 pagesIncreased Intracranial PressureCheryl Lim SorianoPas encore d'évaluation
- Heart Anatomy and Circulatory Systems of Bony FishesDocument10 pagesHeart Anatomy and Circulatory Systems of Bony FishesEj AgsaldaPas encore d'évaluation
- Cardiovascular Anatomy and FunctionsDocument6 pagesCardiovascular Anatomy and FunctionsKerwin LimPas encore d'évaluation
- Hashimoto's Thyroiditis and Its Homeopathic Self Treatment Scheme - Bashir Mahmud ElliasDocument12 pagesHashimoto's Thyroiditis and Its Homeopathic Self Treatment Scheme - Bashir Mahmud ElliasBashir Mahmud Ellias83% (6)
- Understanding Brain Tumors with Medical ImagingDocument46 pagesUnderstanding Brain Tumors with Medical ImagingVo Hong VinhPas encore d'évaluation
- MS.K.49.Pituitary DisordersDocument36 pagesMS.K.49.Pituitary DisordersJuliana Sari HarahapPas encore d'évaluation
- UB Human Physiology Syllabus 2012Document5 pagesUB Human Physiology Syllabus 2012Anonymous MPdGkx87bPas encore d'évaluation
- Lecture: Adrenal DisordersDocument78 pagesLecture: Adrenal DisordersOchendo KingxPas encore d'évaluation
- Basal GangliaDocument29 pagesBasal Gangliaapi-19916399Pas encore d'évaluation
- AVIATION Flight Physiology: - Kirk Michael WebsterDocument56 pagesAVIATION Flight Physiology: - Kirk Michael WebsterabriowaisPas encore d'évaluation
- Approach To Abnormal Liver Enzymes Whitepaper TI 07106Document6 pagesApproach To Abnormal Liver Enzymes Whitepaper TI 07106luceroPas encore d'évaluation
- The Lympho Glandular and Intugmentary System: Presenter: Abdurke Dido - Physician (MD) May 22,2011Document62 pagesThe Lympho Glandular and Intugmentary System: Presenter: Abdurke Dido - Physician (MD) May 22,2011Worku KiflePas encore d'évaluation
- Digestive System Lecture NotesdocxDocument11 pagesDigestive System Lecture NotesdocxAdaPas encore d'évaluation
- HEALTH ASSESSMENT (Ears)Document33 pagesHEALTH ASSESSMENT (Ears)April Mae Magos LabradorPas encore d'évaluation
- Limbic System (Behaviour and Emotion)Document19 pagesLimbic System (Behaviour and Emotion)Patterson MachariaPas encore d'évaluation
- ELS - Q2 - Module 7 - Organ Systems of Representative Animals - V2Document22 pagesELS - Q2 - Module 7 - Organ Systems of Representative Animals - V2Alyza Joy Ramirez100% (6)
- Lactation Nation by Sarah Bird For Texas MonthlyDocument2 pagesLactation Nation by Sarah Bird For Texas MonthlySarah BirdPas encore d'évaluation