Vous aimerez peut-être aussi
- Reflexology For Migraine HeadachesDocument12 pagesReflexology For Migraine Headachescharles100% (1)
- Introduction To Public HealthDocument54 pagesIntroduction To Public HealthKristelle Marie Enanoria Bardon50% (2)
- Blood and Tissue NematodesDocument37 pagesBlood and Tissue NematodesjelenaPas encore d'évaluation
- General Practitioner Sample Resume WWW - Careerfaqs.com - AuDocument3 pagesGeneral Practitioner Sample Resume WWW - Careerfaqs.com - AuSubhash RitwalPas encore d'évaluation
- The Impact of Longitudinal Studies On Understanding Development From Young Adulthood To Old AgeDocument11 pagesThe Impact of Longitudinal Studies On Understanding Development From Young Adulthood To Old AgeLana PeharPas encore d'évaluation
- Histopath Lec (Module 1) : Iintroduction To PathologyDocument17 pagesHistopath Lec (Module 1) : Iintroduction To PathologyAngela ReyesPas encore d'évaluation
- (PMLS) Defining Medical Technology ProfessionDocument3 pages(PMLS) Defining Medical Technology ProfessionBanana BananaPas encore d'évaluation
- General Zoology SyllabusDocument13 pagesGeneral Zoology SyllabusPrecious Bardon-MempinPas encore d'évaluation
- Water AnalysisDocument47 pagesWater AnalysisKyle CollladoPas encore d'évaluation
- Epithelial TissueDocument40 pagesEpithelial TissueTom Anthony TonguiaPas encore d'évaluation
- History of PhlebotomyDocument46 pagesHistory of PhlebotomyDorothy AtilanoPas encore d'évaluation
- Molecular Biology and Diagnostics Course DeliveryDocument34 pagesMolecular Biology and Diagnostics Course DeliveryAbigail Laus100% (2)
- CPH Lab - Prelim TransesDocument4 pagesCPH Lab - Prelim TransesLOUISSE ANNE MONIQUE L. CAYLOPas encore d'évaluation
- Week 2 SolutionsDocument4 pagesWeek 2 Solutionsannavarapuanand100% (2)
- Test Bank For Occupational Therapy in Mental Health A Vision For Participation 2nd Edition Catana Brown Virginia C Stoffel Jaime MunozDocument3 pagesTest Bank For Occupational Therapy in Mental Health A Vision For Participation 2nd Edition Catana Brown Virginia C Stoffel Jaime MunozDavid Ortiz97% (36)
- And The Band Played OnDocument4 pagesAnd The Band Played OnKristelle Marie Enanoria Bardon0% (1)
- Histopathology Lecture 1 Week February 01,2020Document44 pagesHistopathology Lecture 1 Week February 01,2020FatimaMendozaPas encore d'évaluation
- HISTOPATH-MODULE-4 NotesDocument7 pagesHISTOPATH-MODULE-4 NotesKaycee AyoPas encore d'évaluation
- Defining The Practice of Medical Technology or Clinical Laboratory Science ProfessionDocument27 pagesDefining The Practice of Medical Technology or Clinical Laboratory Science ProfessionKianna TicsayPas encore d'évaluation
- Innovations in NursingDocument14 pagesInnovations in NursingDelphy Varghese100% (1)
- CPH Laboratory Exam/Project: Non-Communicable Diseases OR NutritionDocument2 pagesCPH Laboratory Exam/Project: Non-Communicable Diseases OR NutritionteuuuuPas encore d'évaluation
- Capillaria PhilippinenensisDocument4 pagesCapillaria PhilippinenensisnadalabelPas encore d'évaluation
- CPH Medtech TransesDocument10 pagesCPH Medtech TransesBea Janelle E. AfallaPas encore d'évaluation
- Epidemiology in EmergenciesDocument18 pagesEpidemiology in EmergenciessmartisaacPas encore d'évaluation
- TEACHER Healthy Diet American English Upper Intermediate Advanced GroupDocument4 pagesTEACHER Healthy Diet American English Upper Intermediate Advanced GroupMarcus SabiniPas encore d'évaluation
- 2 Public Health For Primary Health CareDocument32 pages2 Public Health For Primary Health CarehervwPas encore d'évaluation
- Reviewer in CPHMDocument8 pagesReviewer in CPHMVianne TabiquePas encore d'évaluation
- Medical Technology Laws AND Bioethics: Imelda A. de Leon, RMT, Mpa ProfessorDocument42 pagesMedical Technology Laws AND Bioethics: Imelda A. de Leon, RMT, Mpa ProfessorMaria ClaraPas encore d'évaluation
- Lesson 1 Introduction History Subfields of Public HealthDocument6 pagesLesson 1 Introduction History Subfields of Public HealthKrixie LagundiPas encore d'évaluation
- Special TopicsDocument8 pagesSpecial Topicskatherine ruizPas encore d'évaluation
- Lesson 1: Community HealthDocument7 pagesLesson 1: Community HealthBianca GeagoniaPas encore d'évaluation
- MEDT02 Lesson 2 - Safety in PhlebotomyDocument5 pagesMEDT02 Lesson 2 - Safety in PhlebotomySHELDY AGONCILLOPas encore d'évaluation
- 6 Ra 1517Document56 pages6 Ra 1517Jay Andrea Vea Dayuday-IsraelPas encore d'évaluation
- Manual AubfDocument4 pagesManual AubfNoraine Princess Tabangcora100% (2)
- Early Beginning of Medical Technology: Vivian HerrickDocument13 pagesEarly Beginning of Medical Technology: Vivian HerrickWho KnowsPas encore d'évaluation
- Psthe 1Document111 pagesPsthe 1Angelica RicoPas encore d'évaluation
- CombinepdfDocument214 pagesCombinepdfAl Ther JumadilPas encore d'évaluation
- PMLS .Docx 1Document9 pagesPMLS .Docx 1ain't your saintessPas encore d'évaluation
- UNIT 3.0 Medical Technology CurriculumDocument12 pagesUNIT 3.0 Medical Technology CurriculumJean Carmelette BalalloPas encore d'évaluation
- Bachelor of Science in Medical Technology 2014Document6 pagesBachelor of Science in Medical Technology 2014Maxine TaeyeonPas encore d'évaluation
- Parasitology Preservation MethodsDocument5 pagesParasitology Preservation MethodsAinah Charina TapicPas encore d'évaluation
- Laboratory Equip: Pipet. It Has Only OneDocument3 pagesLaboratory Equip: Pipet. It Has Only OneAytona Villanueva PearlPas encore d'évaluation
- HISTO-S01-T01-Histology & Its Methods of StudyDocument5 pagesHISTO-S01-T01-Histology & Its Methods of StudyShelahPas encore d'évaluation
- Module # 2 Medical Terminologies and Abbreviations and Ethics in The ProfessionDocument6 pagesModule # 2 Medical Terminologies and Abbreviations and Ethics in The ProfessionJonice NavarroPas encore d'évaluation
- Tests For Dengue GROUP 3Document22 pagesTests For Dengue GROUP 3chocoholic potchiPas encore d'évaluation
- Medical Technology in The Philippines: Problems, Resources, and NeedsDocument24 pagesMedical Technology in The Philippines: Problems, Resources, and NeedsJr BalagtasPas encore d'évaluation
- Histopath Lab ActivityDocument5 pagesHistopath Lab ActivityRakia PillayPas encore d'évaluation
- Ra 5527Document14 pagesRa 5527Kai CulanagPas encore d'évaluation
- Bacte Lec - Prelim ExamDocument84 pagesBacte Lec - Prelim ExamDanielle Anne LambanPas encore d'évaluation
- Chapter 1 - Introduction and History of Medical TechnologyDocument4 pagesChapter 1 - Introduction and History of Medical TechnologyDavid DavidPas encore d'évaluation
- 2017b PDFDocument1 241 pages2017b PDFArizaldo Enriquez CastroPas encore d'évaluation
- Clinical Chemistry I, Syllabus PDFDocument6 pagesClinical Chemistry I, Syllabus PDFAbd ahmadPas encore d'évaluation
- Cc1-Task 4Document8 pagesCc1-Task 4Joshua TrinidadPas encore d'évaluation
- 1 CCHM Trans LecDocument5 pages1 CCHM Trans LecCRUZ, ANNA MARIELLEPas encore d'évaluation
- MT Laws ProjectDocument33 pagesMT Laws ProjectRaymond Sinagpulo VlogPas encore d'évaluation
- Histo ManualDocument16 pagesHisto ManualFitz Gerald CastilloPas encore d'évaluation
- Para-Transes Prelim Exam - Unit 2Document20 pagesPara-Transes Prelim Exam - Unit 2Aysha AishaPas encore d'évaluation
- Lec 1 - IntroductionDocument3 pagesLec 1 - IntroductionHaendra Mae DapilagaPas encore d'évaluation
- CMO14 3mt01Document75 pagesCMO14 3mt01makike100% (2)
- Historical PerspectivesDocument17 pagesHistorical PerspectivesJulius FrondaPas encore d'évaluation
- His Activity PDFDocument15 pagesHis Activity PDFRobinJohnIIPas encore d'évaluation
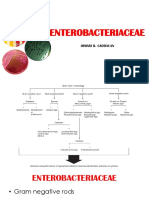
- EXO-Notes JBC ENTEROBACTERIACEAEDocument70 pagesEXO-Notes JBC ENTEROBACTERIACEAECha Tangan-PenolPas encore d'évaluation
- Philippine Blood Banking LawDocument52 pagesPhilippine Blood Banking LawEdgar DumagpiPas encore d'évaluation
- Prelims - GMJ Lecture - Module 2 III DisorderDocument5 pagesPrelims - GMJ Lecture - Module 2 III DisorderjuicePas encore d'évaluation
- Experiment Number 3 Sample Preparation For Blood Banking ProcedureDocument10 pagesExperiment Number 3 Sample Preparation For Blood Banking ProcedureKriziaPas encore d'évaluation
- Principles in Medical Laboratory Science 2Document2 pagesPrinciples in Medical Laboratory Science 2lai cruzPas encore d'évaluation
- Lec - 9 - Residential Occupational Recreational EnvironmentsDocument7 pagesLec - 9 - Residential Occupational Recreational EnvironmentsseaynPas encore d'évaluation
- Para Lec Trans PrelimDocument15 pagesPara Lec Trans PrelimSarah EugenioPas encore d'évaluation
- AphasmidsDocument60 pagesAphasmidsRitz CelsoPas encore d'évaluation
- TOS GenzooDocument5 pagesTOS GenzooKristelle Marie Enanoria BardonPas encore d'évaluation
- ArthopodsDocument66 pagesArthopodsKristelle Marie Enanoria BardonPas encore d'évaluation
- Sexually Trasmitted InfectionsDocument39 pagesSexually Trasmitted InfectionsKristelle Marie Enanoria BardonPas encore d'évaluation
- HormonesDocument3 pagesHormonesKristelle Marie Enanoria BardonPas encore d'évaluation
- House Rules and RegulationsDocument1 pageHouse Rules and RegulationsKristelle Marie Enanoria BardonPas encore d'évaluation
- House Rules and RegulationsDocument1 pageHouse Rules and RegulationsKristelle Marie Enanoria BardonPas encore d'évaluation
- Behavior ChangeDocument9 pagesBehavior ChangeKristelle Marie Enanoria BardonPas encore d'évaluation
- TENTATIVE CLASS LIST (Blank)Document1 pageTENTATIVE CLASS LIST (Blank)Kristelle Marie Enanoria BardonPas encore d'évaluation
- Mycobacteriology Laboratory ManualDocument154 pagesMycobacteriology Laboratory ManualLê Phuong MaiPas encore d'évaluation
- Blank Grading Sheet Lec-LabDocument8 pagesBlank Grading Sheet Lec-LabKristelle Marie Enanoria BardonPas encore d'évaluation
- Ddc-Mls Faculty and StaffDocument2 pagesDdc-Mls Faculty and StaffKristelle Marie Enanoria BardonPas encore d'évaluation
- Antibiotics ResistanceDocument8 pagesAntibiotics ResistanceboredtarteelPas encore d'évaluation
- Antiinflammatorydrugs: Beatriz Monteiro,, Paulo V. SteagallDocument19 pagesAntiinflammatorydrugs: Beatriz Monteiro,, Paulo V. SteagallYohan Oropeza VergaraPas encore d'évaluation
- KEMH Guidelines On Cardiac Disease in PregnancyDocument7 pagesKEMH Guidelines On Cardiac Disease in PregnancyAyesha RazaPas encore d'évaluation
- Bassam Osman ResumeDocument4 pagesBassam Osman ResumeBassam OsmanPas encore d'évaluation
- Prospectus: 1 ReservationsDocument8 pagesProspectus: 1 ReservationsvarunPas encore d'évaluation
- History of Architecture and Town Planning-Course-BrochureDocument42 pagesHistory of Architecture and Town Planning-Course-BrochureSabita AmaniPas encore d'évaluation
- Advanced Cardiovascular Life SupportDocument16 pagesAdvanced Cardiovascular Life SupportSarah Mohd YusofPas encore d'évaluation
- The Chameleon Enthusiast by Noelle SenchynaDocument58 pagesThe Chameleon Enthusiast by Noelle SenchynaDragoș DrăniceanuPas encore d'évaluation
- Current Clinical Strategies: Handbook of AnesthesiologyDocument180 pagesCurrent Clinical Strategies: Handbook of AnesthesiologydramaganaPas encore d'évaluation
- These - Are - The - 41 - Thread - by - Morpheusresist - Sep 6, 22 - From - RattibhaDocument10 pagesThese - Are - The - 41 - Thread - by - Morpheusresist - Sep 6, 22 - From - RattibhaRohan MPas encore d'évaluation
- Pengaruh Metode Pengeringan Terhadap Karakter Mutu Fisik Dan Kimia Serbuk Minuman Instan Kulit Buah NagaDocument9 pagesPengaruh Metode Pengeringan Terhadap Karakter Mutu Fisik Dan Kimia Serbuk Minuman Instan Kulit Buah NagaHadi Yusuf FaturochmanPas encore d'évaluation
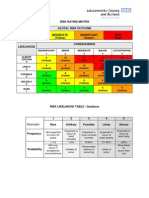
- Example of A NHS Risk Rating MatrixDocument2 pagesExample of A NHS Risk Rating MatrixRochady SetiantoPas encore d'évaluation
- Pecial Eature: Transitions in Pharmacy Practice, Part 3: Effecting Change-The Three-Ring CircusDocument7 pagesPecial Eature: Transitions in Pharmacy Practice, Part 3: Effecting Change-The Three-Ring CircusSean BlackmerPas encore d'évaluation
- 2018 MUSE Inspire Conference - Show and Tell SessionsDocument13 pages2018 MUSE Inspire Conference - Show and Tell SessionsMichele LambertPas encore d'évaluation
- Sq20-030 - Fact Sheet - Informed Consent - Nsqhs-8.9aDocument4 pagesSq20-030 - Fact Sheet - Informed Consent - Nsqhs-8.9aPedro Medeiros JrPas encore d'évaluation
- Aravind Eye Care Systems: Providing Total Eye Care To The Rural PopulationDocument13 pagesAravind Eye Care Systems: Providing Total Eye Care To The Rural PopulationAvik BorahPas encore d'évaluation
- PneumoconiosisDocument19 pagesPneumoconiosisgabriela.was.gabbbiePas encore d'évaluation
- Interpretation: LPL - PSC Chandigarh Sector 19-D Booth No:-3, Sector:-19-D ChandigarhDocument5 pagesInterpretation: LPL - PSC Chandigarh Sector 19-D Booth No:-3, Sector:-19-D ChandigarhSanPas encore d'évaluation
- PNA 2012 National Convention LectureDocument60 pagesPNA 2012 National Convention LectureHarby Ongbay AbellanosaPas encore d'évaluation
- Laparoscopic Appendectomy SurgeryDocument2 pagesLaparoscopic Appendectomy SurgeryNycoPas encore d'évaluation
- Lab Report 15438869 20231127064225Document1 pageLab Report 15438869 20231127064225carilloabhe21Pas encore d'évaluation
- The 10 Most (And Least) Prestigious Jobs in AmericaDocument12 pagesThe 10 Most (And Least) Prestigious Jobs in AmericaParlindungan PardedePas encore d'évaluation
- Pappas Bikhazi 2023 Babe Ruth S Anaplastic Epidermoid Carcinoma of The NasopharynxDocument5 pagesPappas Bikhazi 2023 Babe Ruth S Anaplastic Epidermoid Carcinoma of The NasopharynxVinoster ProductionPas encore d'évaluation