Vous aimerez peut-être aussi
- CholecystitisDocument10 pagesCholecystitisKamilatun NiamahPas encore d'évaluation
- 6.1 Pitutary DisorderDocument32 pages6.1 Pitutary Disordersiltanu awokePas encore d'évaluation
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- 5 Acute Cholecystitis - Libre PathologyDocument5 pages5 Acute Cholecystitis - Libre Pathologyfado100% (1)
- A Simple Guide to Hyperaldosteronism, Diagnosis, Treatment and Related ConditionsD'EverandA Simple Guide to Hyperaldosteronism, Diagnosis, Treatment and Related ConditionsPas encore d'évaluation
- Ali - CNS InfectionsDocument129 pagesAli - CNS InfectionsMichael BortzPas encore d'évaluation
- Chronic CholecystitisDocument7 pagesChronic CholecystitisErika alfonsoPas encore d'évaluation
- Cerebral EdemaDocument21 pagesCerebral EdemasridharPas encore d'évaluation
- 9 Mesenchymal Tumors 2Document77 pages9 Mesenchymal Tumors 2Ther Ray100% (1)
- Plasma Cell DyscrasiaDocument45 pagesPlasma Cell DyscrasiaAymen OmerPas encore d'évaluation
- SBL100-Immunology Lectures 1-3Document92 pagesSBL100-Immunology Lectures 1-3B.simhachalam100% (1)
- Central Nervous System AbnormalitiesDocument56 pagesCentral Nervous System AbnormalitiesApin PokhrelPas encore d'évaluation
- Cerebrovascular Pathology: Abel B. (MD) Pathology Lectures, NMEI, DBUDocument59 pagesCerebrovascular Pathology: Abel B. (MD) Pathology Lectures, NMEI, DBUdenekePas encore d'évaluation
- Pituitary Tumors Engleza 2Document89 pagesPituitary Tumors Engleza 2Achmad Harun MuchsinPas encore d'évaluation
- Cerebro Vascular AccidentDocument82 pagesCerebro Vascular AccidentJayvee Novenario Casaljay100% (1)
- Check Unit 557 Jan-Feb Genetics v3 PDFDocument36 pagesCheck Unit 557 Jan-Feb Genetics v3 PDFdragon66Pas encore d'évaluation
- Thrombosis and EmbolismDocument39 pagesThrombosis and Embolismilva100% (1)
- Ophthalmology - Passmedicine 2012 - 62013146Document18 pagesOphthalmology - Passmedicine 2012 - 62013146abuahmed&janaPas encore d'évaluation
- Systolic Dysfunction:: Types of Heart FailureDocument13 pagesSystolic Dysfunction:: Types of Heart FailureElisabeth F. OjhaPas encore d'évaluation
- University of Cape Coasst: Mls303A: Microbiology IiiDocument31 pagesUniversity of Cape Coasst: Mls303A: Microbiology IiiErnest KyerePas encore d'évaluation
- Endocrine System: THE Adrenal GlandsDocument50 pagesEndocrine System: THE Adrenal GlandsAbdel Aziz NazihPas encore d'évaluation
- NEPHROTIC SYNDROME - HamidDocument20 pagesNEPHROTIC SYNDROME - HamidAbdul Hamid OmarPas encore d'évaluation
- NephroticDocument8 pagesNephroticsangheetaPas encore d'évaluation
- HivDocument36 pagesHivfenendriyaniPas encore d'évaluation
- Glomerulonephritis 2019Document31 pagesGlomerulonephritis 2019EsoklailPas encore d'évaluation
- Acute Urinary ObstructionDocument34 pagesAcute Urinary ObstructionHafizur RashidPas encore d'évaluation
- Vasculitis: Disorder Vessels Pathology Presentation Test TX OtherDocument3 pagesVasculitis: Disorder Vessels Pathology Presentation Test TX OthermcwnotesPas encore d'évaluation
- Common Parathyroid Disorders in Children: DR Sarar MohamedDocument47 pagesCommon Parathyroid Disorders in Children: DR Sarar MohamedTirou100% (1)
- Mycosis Systemik - Blok TID - Feb 2015Document67 pagesMycosis Systemik - Blok TID - Feb 2015Kiki Celiana TiffanyPas encore d'évaluation
- Leg UlcerDocument28 pagesLeg UlcerRanindya PutriPas encore d'évaluation
- Cns InfectionsDocument141 pagesCns InfectionsReda AlyPas encore d'évaluation
- Presented By:: Ali Jaber Al-Faifi Salman NasserDocument23 pagesPresented By:: Ali Jaber Al-Faifi Salman NasserCalvin PrasetioPas encore d'évaluation
- Adrenal GlandDocument47 pagesAdrenal GlandsuthaPas encore d'évaluation
- Nephrotic Syndrome 2016Document45 pagesNephrotic Syndrome 2016alaaPas encore d'évaluation
- Hem-Onc: AnswerDocument3 pagesHem-Onc: AnswerAman Raj KPas encore d'évaluation
- Valvular Heart DseDocument8 pagesValvular Heart DseJane Pineda CuraPas encore d'évaluation
- Neurological Manifestations of HIVDocument34 pagesNeurological Manifestations of HIVashuPas encore d'évaluation
- InflammationDocument41 pagesInflammationbharath goPas encore d'évaluation
- Nephrotic Syndrome: Jaiganesh.M, M.D (General Medicine) Asst. Professor, S.M.C.HDocument60 pagesNephrotic Syndrome: Jaiganesh.M, M.D (General Medicine) Asst. Professor, S.M.C.HJaiganesh MuruganandamPas encore d'évaluation
- Basic Pathological Aspects of Nervous SystemDocument72 pagesBasic Pathological Aspects of Nervous SystemFariz FadhlurrahmanPas encore d'évaluation
- Acute Renal FailureDocument5 pagesAcute Renal FailureSalman KhanPas encore d'évaluation
- Pathology of Cns InfectionsDocument39 pagesPathology of Cns Infectionsskin_docPas encore d'évaluation
- Basal Cell Carcinoma, Pilar Type (Keratotic Basal Cell Carcinoma)Document7 pagesBasal Cell Carcinoma, Pilar Type (Keratotic Basal Cell Carcinoma)Deba P SarmaPas encore d'évaluation
- Acute CNS Infections: James E. Peacock, Jr. MDDocument53 pagesAcute CNS Infections: James E. Peacock, Jr. MDEhab KhiryPas encore d'évaluation
- Alopecia AreataDocument71 pagesAlopecia AreatadrbhaveshpPas encore d'évaluation
- 05 - Respiratory Pathology 2 (25 Min)Document25 pages05 - Respiratory Pathology 2 (25 Min)Felix Miquel AcostaPas encore d'évaluation
- Neuro General Neuro: Proptosis/ Exophthalmos ChemosisDocument4 pagesNeuro General Neuro: Proptosis/ Exophthalmos ChemosisShakina FareedPas encore d'évaluation
- Hyper para Thyroid Is MDocument27 pagesHyper para Thyroid Is MIbrahimWagesPas encore d'évaluation
- Acute Bacterial MeningitisDocument49 pagesAcute Bacterial MeningitisKumara GuruPas encore d'évaluation
- CNS Infection 11Document75 pagesCNS Infection 11Paulo Josue SabladPas encore d'évaluation
- Course: Medical Surgical Nursing Ii Course Code: NSC 322 Topic: Leukamia Lecturer: Mrs Chukwu Date: Tuesday, 7Th June, 2022Document13 pagesCourse: Medical Surgical Nursing Ii Course Code: NSC 322 Topic: Leukamia Lecturer: Mrs Chukwu Date: Tuesday, 7Th June, 2022Leo D' GreatPas encore d'évaluation
- HIV Natural HistoryDocument10 pagesHIV Natural HistoryNirav Sharma100% (1)
- Practical Pathology - GoiterDocument8 pagesPractical Pathology - GoiterAdlina TajuddinPas encore d'évaluation
- Aplastic AnaemiaDocument21 pagesAplastic AnaemiaAbhinav ReddyPas encore d'évaluation
- Kidney NewDocument4 pagesKidney NewParth BhayanaPas encore d'évaluation
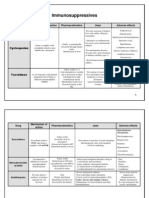
- 1 - Immuno Tables1Document4 pages1 - Immuno Tables1Urugonda VenumadhavPas encore d'évaluation
- Nephrotic SyndromeDocument24 pagesNephrotic SyndromeJawad SaleemPas encore d'évaluation
- Vasculitis - Student Notes Tabulated2Document2 pagesVasculitis - Student Notes Tabulated2Kirstie de LunaPas encore d'évaluation
- Tutoría Académica - Etapas Clases OnlineDocument8 pagesTutoría Académica - Etapas Clases OnlineSol CamusPas encore d'évaluation
- A Method of Comparing The Areas Under Receiver Operating: Characteristic Curves Derived FromDocument5 pagesA Method of Comparing The Areas Under Receiver Operating: Characteristic Curves Derived FromJorgelino João GuterresPas encore d'évaluation
- Tests For Two ROC Curves: PASS Sample Size SoftwareDocument16 pagesTests For Two ROC Curves: PASS Sample Size SoftwareSol CamusPas encore d'évaluation
- Derivation Vs ValidationDocument3 pagesDerivation Vs ValidationSol CamusPas encore d'évaluation
- Krok 1 Medicine 2020 Papers MCQ Practice - OnlineKitaabsDocument48 pagesKrok 1 Medicine 2020 Papers MCQ Practice - OnlineKitaabsHarsh NimavatPas encore d'évaluation
- OIL SyllabusDocument40 pagesOIL SyllabusAbhishekPas encore d'évaluation
- Histopathology Photos - Part 1Document86 pagesHistopathology Photos - Part 1solom islamPas encore d'évaluation
- VASCULITIS by Dr. AJ. 1Document34 pagesVASCULITIS by Dr. AJ. 1Abira KhanPas encore d'évaluation
- Harper S Textbook of Pediatric Dermatology - 2019 - Hoeger - Front MatterDocument34 pagesHarper S Textbook of Pediatric Dermatology - 2019 - Hoeger - Front MatteryelsiPas encore d'évaluation
- Self Assessment CasesDocument512 pagesSelf Assessment CasesmixandgoPas encore d'évaluation
- Identification of Basic Patterns - Skin - Peri-Infundibulitis and PerifolliculitisDocument24 pagesIdentification of Basic Patterns - Skin - Peri-Infundibulitis and PerifolliculitisBogdan CarabasPas encore d'évaluation
- Chronic GastritisDocument37 pagesChronic GastritisBondu Babu007Pas encore d'évaluation
- Jurnal Infeksi Saluran PencernaanDocument22 pagesJurnal Infeksi Saluran PencernaanDini Okta PutriPas encore d'évaluation
- Harper S Textbook of Pediatric Dermatology Wiley Blackwell 2020 PDFDocument2 511 pagesHarper S Textbook of Pediatric Dermatology Wiley Blackwell 2020 PDFAlinaPas encore d'évaluation
- Diagnosis of Small Lung Biopsy An Integrated Approach by Mostafa M. FraigDocument111 pagesDiagnosis of Small Lung Biopsy An Integrated Approach by Mostafa M. FraigFlaviaPas encore d'évaluation
- A Summary of LeprosyDocument80 pagesA Summary of LeprosyJohnPas encore d'évaluation
- Inflammation and Repair Wound HealingDocument29 pagesInflammation and Repair Wound Healingakshay dhootPas encore d'évaluation
- Tests General 08Document32 pagesTests General 08melvingeorge200950% (2)
- Pathology Slides by Organ 2Document25 pagesPathology Slides by Organ 2Lin AdutPas encore d'évaluation
- Hi-Yield Notes in SurgeryDocument18 pagesHi-Yield Notes in SurgeryJohn Christopher Luces50% (2)
- Giant Cell Epulis: Report of 2 Cases.: Oral PathologyDocument11 pagesGiant Cell Epulis: Report of 2 Cases.: Oral PathologyVheen Dee DeePas encore d'évaluation
- Wegener GranulomatosisDocument3 pagesWegener GranulomatosisShandyfauzyPas encore d'évaluation
- AssDocument5 pagesAssAlona Argie PianoPas encore d'évaluation
- Inflammation: Cardinal Signs of InflammationDocument9 pagesInflammation: Cardinal Signs of InflammationGeoffreyPas encore d'évaluation
- Anatomy and Histology of The Normal Lung and AirwaysDocument20 pagesAnatomy and Histology of The Normal Lung and AirwaysFahd Abdullah Al-refaiPas encore d'évaluation
- Macroscopic Diagnostic For Pathoanathomy and Cytopathology ExamDocument21 pagesMacroscopic Diagnostic For Pathoanathomy and Cytopathology Examkapil pancholiPas encore d'évaluation
- Beaman B.L. & Beaman L. 1994. Nocardia Species - Host-Parasite Relationships. 1Document52 pagesBeaman B.L. & Beaman L. 1994. Nocardia Species - Host-Parasite Relationships. 1Arthur PiresPas encore d'évaluation
- Gingival EnlargementDocument125 pagesGingival Enlargementdr_saurabhsinha_165Pas encore d'évaluation
- Ciri Khas Histo PADocument28 pagesCiri Khas Histo PAFitria SartikaPas encore d'évaluation
- Actinobacillosis &actinomycosisDocument16 pagesActinobacillosis &actinomycosisVickypathoPas encore d'évaluation
- Tutorial Skenario A Blok 14 (PPT)Document75 pagesTutorial Skenario A Blok 14 (PPT)Prasetya AnugrahPas encore d'évaluation
- Leprosy: Elizabeth Bizuneh M.D Consultant DermatologistDocument59 pagesLeprosy: Elizabeth Bizuneh M.D Consultant DermatologistAustine OsawePas encore d'évaluation
- MCQ 2Document22 pagesMCQ 2Mohmmad WhaidyPas encore d'évaluation
- Vascular DiseasesDocument9 pagesVascular DiseasesJose SirittPas encore d'évaluation