Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Carbohydrate Metabolism McKee Chapter8Document44 pagesCarbohydrate Metabolism McKee Chapter8David SeidelPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Insulin and Glucagon HormonesDocument42 pagesInsulin and Glucagon HormonesRosePas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Biochemistry: Introduction To MetabolismDocument7 pagesBiochemistry: Introduction To MetabolismAria ScribePas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Fed State of MetabolismDocument40 pagesFed State of MetabolismBHARANIDHARAN M.VPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Integration of MetabolismDocument51 pagesIntegration of MetabolismKaif AliPas encore d'évaluation
- Nutrition and MetabolismDocument179 pagesNutrition and MetabolismTuTitPas encore d'évaluation
- Medicinal Biochemistry 1st Pharm D Quistion BankDocument7 pagesMedicinal Biochemistry 1st Pharm D Quistion BankAnanda Vijayasarathy0% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- MLT Revised Curriculum (U) 19-12-2019 (Final Version)Document86 pagesMLT Revised Curriculum (U) 19-12-2019 (Final Version)Fawad SawabiPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Biochm AIMC 2nd YrDocument14 pagesBiochm AIMC 2nd YrAurang ZaibPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- PancreasDocument17 pagesPancreassanathPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Biochemistry 090819Document26 pagesBiochemistry 090819Shubham GusingePas encore d'évaluation
- Clinical Chemistry ReviewerDocument29 pagesClinical Chemistry ReviewerbokbokbokPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- BiochemistryDocument135 pagesBiochemistryPradip HamalPas encore d'évaluation
- Biochemistry of CVSDocument311 pagesBiochemistry of CVSAsne ManPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Fulltext01 PDFDocument92 pagesFulltext01 PDFغاز الشمالPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Biochemistry (Paper VI)Document8 pagesBiochemistry (Paper VI)Shahidullah Kaisar ShovonPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Carbohydrates: Biochemistry and Clinical Significance: Prof. Fritz Von T. Gella, RMT, MD October 5, 2021Document10 pagesCarbohydrates: Biochemistry and Clinical Significance: Prof. Fritz Von T. Gella, RMT, MD October 5, 2021May Ann EnoserioPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Functions of CarbohydratesDocument14 pagesFunctions of CarbohydratesRenu SharmaPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Student Notes: Clinchem1: Davao Doctors College Medical Laboratory Science DepartmentDocument9 pagesStudent Notes: Clinchem1: Davao Doctors College Medical Laboratory Science DepartmentMelody Jane PardilloPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Chapter 18 HandoutDocument8 pagesChapter 18 HandoutreynandPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- 3cce171c-d4d7-49b0-8dda-425b225fb1f5 (1)Document2 pages3cce171c-d4d7-49b0-8dda-425b225fb1f5 (1)j4606074Pas encore d'évaluation
- Course Syllabus and Schedule: College of Science University of The Philippines Diliman, Quezon City 1101Document4 pagesCourse Syllabus and Schedule: College of Science University of The Philippines Diliman, Quezon City 1101Ruth Danielle Gascon0% (1)
- Testbank MetabolismDocument11 pagesTestbank MetabolismRiky Ikhwan50% (2)
- 100 MCAT TipsDocument23 pages100 MCAT TipsJhilianne Batino100% (1)
- CARBOHYDRATE METABOLISM Part II (Glycolysis)Document9 pagesCARBOHYDRATE METABOLISM Part II (Glycolysis)InshaPas encore d'évaluation
- Antidiabetic Drugs: Raymund N. Tapaoan, RPHDocument23 pagesAntidiabetic Drugs: Raymund N. Tapaoan, RPHNicole EncinaresPas encore d'évaluation
- Nikhil BTP Mid Term ReportDocument17 pagesNikhil BTP Mid Term ReportNikhil SaiyamPas encore d'évaluation
- Name: Santos, Lore Anne Mhae T. Date: - Instructor: Giovanni D. David, Edd, RN ScoreDocument4 pagesName: Santos, Lore Anne Mhae T. Date: - Instructor: Giovanni D. David, Edd, RN ScoreLore Anne Mhae SantosPas encore d'évaluation
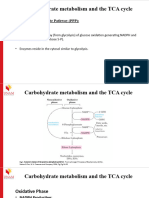
- Carbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Document17 pagesCarbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Frolian MichaelPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Rosenbaum Et Al-2019-ObesityDocument12 pagesRosenbaum Et Al-2019-ObesityaloverofdancePas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)