Vous aimerez peut-être aussi
- AtorvastatinDocument27 pagesAtorvastatinBolgam PradeepPas encore d'évaluation
- CRESTOR Launch Presentation January 2011Document40 pagesCRESTOR Launch Presentation January 2011Chikezie Onwukwe67% (3)
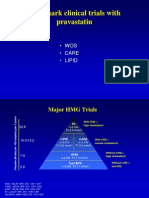
- Wos Care LipidDocument55 pagesWos Care LipidJuliana FeronPas encore d'évaluation
- Aztor Cme NewDocument59 pagesAztor Cme NewSheikh Sharfuddin RajeevPas encore d'évaluation
- Lipid Management in The Diabetic PatientDocument32 pagesLipid Management in The Diabetic PatientJezza Estévez VarelaPas encore d'évaluation
- Pharm 316 Case Presentation: Statins in The Golden Years - Statin For Primary Prevention in ElderlyDocument37 pagesPharm 316 Case Presentation: Statins in The Golden Years - Statin For Primary Prevention in ElderlyKevin JiaPas encore d'évaluation
- JNC VIII Hypertension SaudiDocument47 pagesJNC VIII Hypertension SaudiDavid Chandra EriksonPas encore d'évaluation
- Lipid Management in DMDocument33 pagesLipid Management in DMSheung WongPas encore d'évaluation
- 6 Studii StatineDocument37 pages6 Studii Statinejust4uhopePas encore d'évaluation
- The MERCURY I OpenDocument12 pagesThe MERCURY I OpenSharmil IyapillaiPas encore d'évaluation
- DyslipidemiaManagement Continuum 2011Document13 pagesDyslipidemiaManagement Continuum 2011Zuleika DöObsönPas encore d'évaluation
- Can The Ketogenic Diet Favorably Modify Cardiovascular Disease Risk Factors?Document27 pagesCan The Ketogenic Diet Favorably Modify Cardiovascular Disease Risk Factors?Prav GrewalPas encore d'évaluation
- Diabetes and Vascular Disease Research 2010 Younis 289 95Document8 pagesDiabetes and Vascular Disease Research 2010 Younis 289 95Marthin HotangPas encore d'évaluation
- Cardio Metabolic Risk in DiabetesDocument29 pagesCardio Metabolic Risk in DiabetesoctoindradjajaPas encore d'évaluation
- 2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"Document51 pages2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"dr_yasserPas encore d'évaluation
- Original Article: Journal of Clinical Lipidology (2017)Document12 pagesOriginal Article: Journal of Clinical Lipidology (2017)IrhamPas encore d'évaluation
- Perhitungan RRDocument5 pagesPerhitungan RRMuh Witly FairussaflyPas encore d'évaluation
- Comparative Effects of LO-mg Versus 80-Mg Atorvastatin On High-Sensitivity C-Reactive ProteinDocument16 pagesComparative Effects of LO-mg Versus 80-Mg Atorvastatin On High-Sensitivity C-Reactive ProteinferdianriskaPas encore d'évaluation
- European Journal of Preventive Cardiology-2016-Karlson-744-7 PDFDocument4 pagesEuropean Journal of Preventive Cardiology-2016-Karlson-744-7 PDFIrina Cabac-PogoreviciPas encore d'évaluation
- Selecting Successful Lipid-Lowering Treatments: James M. Mckenney, PharmdDocument31 pagesSelecting Successful Lipid-Lowering Treatments: James M. Mckenney, Pharmdja30jd15ve15an22Pas encore d'évaluation
- TrajentaDocument23 pagesTrajentamonicaolivinePas encore d'évaluation
- Metabolik SindromeDocument46 pagesMetabolik SindromePAn Lover'zPas encore d'évaluation
- MRCP 2 Clinical Trial Data MRCP 2Document5 pagesMRCP 2 Clinical Trial Data MRCP 2Yong Fang YuePas encore d'évaluation
- 2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummaryDocument77 pages2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummaryBetsy Brown ByersmithPas encore d'évaluation
- 2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/ Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummaryDocument77 pages2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/ Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummarydanielPas encore d'évaluation
- Objective:: BackgroundDocument23 pagesObjective:: BackgroundJanine DimaangayPas encore d'évaluation
- Efek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularDocument6 pagesEfek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularAndrie WigunaPas encore d'évaluation
- Catalano1992 PDFDocument6 pagesCatalano1992 PDFSepti Fadhilah SPPas encore d'évaluation
- 27 FullDocument6 pages27 FullKrishna R KhanalPas encore d'évaluation
- 13.rajasekar Research ArticleDocument9 pages13.rajasekar Research ArticleBaru Chandrasekhar RaoPas encore d'évaluation
- AntioksidanDocument5 pagesAntioksidanRakasiwi GalihPas encore d'évaluation
- Atorvastatin Statin in CVD ManagementDocument37 pagesAtorvastatin Statin in CVD ManagementSriPas encore d'évaluation
- Statins in CVD Management: Is Just Lipid Lowering Enough?Document37 pagesStatins in CVD Management: Is Just Lipid Lowering Enough?SriPas encore d'évaluation
- Jurnal 4 WordDocument20 pagesJurnal 4 WordSri MaryatiPas encore d'évaluation
- Understanding The Needs of The High Productive DyslipidemiaDocument47 pagesUnderstanding The Needs of The High Productive DyslipidemiachchchchkPas encore d'évaluation
- Dyslipidaemia 2019Document61 pagesDyslipidaemia 2019fatima.shqeratPas encore d'évaluation
- Effects of Niacin Combination Therapy With Statin or Bile-Acid Resin On Lipoproteins and Cardiovascular DiseaseDocument10 pagesEffects of Niacin Combination Therapy With Statin or Bile-Acid Resin On Lipoproteins and Cardiovascular Diseaselina budiartiPas encore d'évaluation
- AMADEO Full PaperDocument6 pagesAMADEO Full PaperAnggraeni PermatasariPas encore d'évaluation
- Jurnal MaglitinideDocument7 pagesJurnal MaglitinideWanda Novia P SPas encore d'évaluation
- HopeDocument21 pagesHopeIsnawan WidyayantoPas encore d'évaluation
- Evolve Study Journal Club PresentationDocument62 pagesEvolve Study Journal Club PresentationsantoshvellorePas encore d'évaluation
- Statistical Report IHNDocument7 pagesStatistical Report IHNvanigvPas encore d'évaluation
- Hyperlipidemia: Brian V. Reamy, MD, Colonel, USAF, MC Chair - Department of Family Medicine Uniformed Services UniversityDocument58 pagesHyperlipidemia: Brian V. Reamy, MD, Colonel, USAF, MC Chair - Department of Family Medicine Uniformed Services Universityayloleh87Pas encore d'évaluation
- Lipids JBDocument48 pagesLipids JBMuvenn KannanPas encore d'évaluation
- From Evidence Based To Clinical Practice in Type 2 Diabetes MellitusDocument40 pagesFrom Evidence Based To Clinical Practice in Type 2 Diabetes MellitusscribdPas encore d'évaluation
- Lipid Management For The Prevention of Atherosclerotic Cardiovascular DiseaseDocument6 pagesLipid Management For The Prevention of Atherosclerotic Cardiovascular DiseaseemirkurtalicPas encore d'évaluation
- Dapagliflozin - Effect On Uric AcidDocument4 pagesDapagliflozin - Effect On Uric AcidCintia TakedaPas encore d'évaluation
- Sonu B ReportDocument7 pagesSonu B ReportSaujanyaSengarPas encore d'évaluation
- NursingresearchreportDocument12 pagesNursingresearchreportapi-300699057Pas encore d'évaluation
- RosuvastatinDocument62 pagesRosuvastatinEileen del RosarioPas encore d'évaluation
- Diabetes Management UpdateDocument64 pagesDiabetes Management UpdatethisarPas encore d'évaluation
- Dr. Esperanza Cabral ModuleDocument54 pagesDr. Esperanza Cabral ModuleNazarine TorresPas encore d'évaluation
- Heart Diseases: An Overview On Clinical Trials: Dr. Khaled Dhifullah Al-Harby Consultant Family PhysicianDocument68 pagesHeart Diseases: An Overview On Clinical Trials: Dr. Khaled Dhifullah Al-Harby Consultant Family PhysicianalghaidanyPas encore d'évaluation
- Role of Rosuvastatin in The Treatment of DyslipidemiaDocument16 pagesRole of Rosuvastatin in The Treatment of DyslipidemiaabcdefPas encore d'évaluation
- Effectiveness and Safety of Low-Dose Pravastatin and Squalene, Alone and in Combination, in Elderly Patients With HypercholesterolemiaDocument6 pagesEffectiveness and Safety of Low-Dose Pravastatin and Squalene, Alone and in Combination, in Elderly Patients With HypercholesterolemiaeduardochocincoPas encore d'évaluation
- CLC 4960230910Document7 pagesCLC 4960230910walnut21Pas encore d'évaluation
- Nutraceuticals and Human Blood Platelet Function: Applications in Cardiovascular HealthD'EverandNutraceuticals and Human Blood Platelet Function: Applications in Cardiovascular HealthPas encore d'évaluation
- Common Diagnostic Therapeutic Injections of The Foot Ankle by Jacob Sellon MD PDFDocument61 pagesCommon Diagnostic Therapeutic Injections of The Foot Ankle by Jacob Sellon MD PDFNovianWibowoDokterPas encore d'évaluation
- Greater Occipital NeuralgiaDocument10 pagesGreater Occipital NeuralgiaNovianWibowoDokter100% (1)
- Alvarez Hypertension PDFDocument99 pagesAlvarez Hypertension PDFmeliani.fitriPas encore d'évaluation
- Manual Book ToshibaDocument218 pagesManual Book ToshibaanrihmPas encore d'évaluation
- Management of Acute Ischemic StrokeDocument22 pagesManagement of Acute Ischemic StrokeAn-Nisa Khoirun UmmiPas encore d'évaluation
- Common Diagnostic Therapeutic Injections of The Foot Ankle by Jacob Sellon MDDocument61 pagesCommon Diagnostic Therapeutic Injections of The Foot Ankle by Jacob Sellon MDNovianWibowoDokterPas encore d'évaluation
- Caudal Epidural 2000 3 305-312Document8 pagesCaudal Epidural 2000 3 305-312NovianWibowoDokterPas encore d'évaluation
- IMT IndexDocument11 pagesIMT IndexNovianWibowoDokterPas encore d'évaluation
- Management of Acute Ischemic StrokeDocument10 pagesManagement of Acute Ischemic StrokeNovianWibowoDokterPas encore d'évaluation
- Caudal Epidural 2000 3 305-312Document8 pagesCaudal Epidural 2000 3 305-312NovianWibowoDokterPas encore d'évaluation
- HomosisteinDocument9 pagesHomosisteinAffan Sodiq Sabda PrayogaPas encore d'évaluation
- Diacerein: A New Symptomatic Slow Acting Drug For OsteoarthritisDocument3 pagesDiacerein: A New Symptomatic Slow Acting Drug For OsteoarthritisNovianWibowoDokterPas encore d'évaluation
- Chronic Bronchitis Chapter 11Document43 pagesChronic Bronchitis Chapter 11NovianWibowoDokterPas encore d'évaluation
- Chronic Bronchitis Chapter 11Document43 pagesChronic Bronchitis Chapter 11NovianWibowoDokterPas encore d'évaluation
- Diazepam Infus PDFDocument7 pagesDiazepam Infus PDFNovianWibowoDokterPas encore d'évaluation
- Alvarez Hypertension PDFDocument99 pagesAlvarez Hypertension PDFmeliani.fitriPas encore d'évaluation
- Alvarez Hypertension PDFDocument99 pagesAlvarez Hypertension PDFmeliani.fitriPas encore d'évaluation
- Nicardipine (Cardene ®) - Intravenous (IV) Dilution PDFDocument3 pagesNicardipine (Cardene ®) - Intravenous (IV) Dilution PDFNovianWibowoDokterPas encore d'évaluation
- Neuropathic Pain SlidesDocument28 pagesNeuropathic Pain SlidesAndrias Oz100% (1)
- Cavernous Sinus Thrombosis - PDFDocument4 pagesCavernous Sinus Thrombosis - PDFNovianWibowoDokterPas encore d'évaluation
- Cavernous Sinus Thrombosis - PDFDocument4 pagesCavernous Sinus Thrombosis - PDFNovianWibowoDokterPas encore d'évaluation
- Wellness Check PrintableDocument2 pagesWellness Check PrintablethubtendrolmaPas encore d'évaluation
- Biokimia NeurupsikiatriDocument40 pagesBiokimia Neurupsikiatrisuyudi kimikoPas encore d'évaluation
- Ethical Dilemmas in The Practice of NursingDocument15 pagesEthical Dilemmas in The Practice of Nursingestudiant9Pas encore d'évaluation
- Blood Typing GameDocument4 pagesBlood Typing GameWidjaya HS TeacherPas encore d'évaluation
- Congenital HypothyroidismDocument36 pagesCongenital HypothyroidismRandi DwiyantoPas encore d'évaluation
- Legg-Calvé-Perthes Disease: Roberto E. Novo, DVM, DACVSDocument2 pagesLegg-Calvé-Perthes Disease: Roberto E. Novo, DVM, DACVSEdi BackyPas encore d'évaluation
- Interpretation of Histograms and Its Correlation WDocument5 pagesInterpretation of Histograms and Its Correlation WrezqiPas encore d'évaluation
- Conversation Bhs Inggris Untuk 5 OrangDocument4 pagesConversation Bhs Inggris Untuk 5 OrangKurogami100% (1)
- Ayuvediya Approch Toward Iron Deficiency Anaemia - A Case StudyDocument4 pagesAyuvediya Approch Toward Iron Deficiency Anaemia - A Case StudyIJAR JOURNALPas encore d'évaluation
- Cervical Cancer and Human Papillomavirus: HearingDocument596 pagesCervical Cancer and Human Papillomavirus: HearingScribd Government DocsPas encore d'évaluation
- Daniels and Jenkins - Therapy With Children 2e PDFDocument2 pagesDaniels and Jenkins - Therapy With Children 2e PDFloubwoyPas encore d'évaluation
- @MedicalBooksStore 2015 Office Based PDFDocument237 pages@MedicalBooksStore 2015 Office Based PDFGalih WicaksonoPas encore d'évaluation
- Case GNApsDocument47 pagesCase GNApsAndhika Hadi WirawanPas encore d'évaluation
- Jurnal OnlineDocument5 pagesJurnal OnlineWireifnitedPas encore d'évaluation
- A Literary LifeDocument5 pagesA Literary LifeLayla AliPas encore d'évaluation
- An Industrial Training Report at Biogenetic Drugs PVT - Ltd. Baddi (H.P.)Document26 pagesAn Industrial Training Report at Biogenetic Drugs PVT - Ltd. Baddi (H.P.)pankajsinghal27010% (2)
- Medical Bill 2Document1 pageMedical Bill 2arun_ioclPas encore d'évaluation
- Strengths Based NursingDocument22 pagesStrengths Based NursingTHOHAROH0% (1)
- LydiaDocument219 pagesLydiatayabakhanPas encore d'évaluation
- Hydralazine Drug StudyDocument1 pageHydralazine Drug Studymilkv71% (7)
- Case 3 Tuberculosis Group 3Document72 pagesCase 3 Tuberculosis Group 3Antonio EscotoPas encore d'évaluation
- Nonsurgical Treatment of Chronic Anal Fissure: Nitroglycerin and Dilatation Versus Nifedipine and Botulinum ToxinDocument5 pagesNonsurgical Treatment of Chronic Anal Fissure: Nitroglycerin and Dilatation Versus Nifedipine and Botulinum Toxinsheik lalPas encore d'évaluation
- Nursing Information SystemDocument20 pagesNursing Information SystemShahad Hakimuddin100% (1)
- Oral CavityDocument79 pagesOral CavityueumanaPas encore d'évaluation
- Final Announcement - 6721760944 PDFDocument23 pagesFinal Announcement - 6721760944 PDFthifla farhaniPas encore d'évaluation
- 70000769rev.2ecube7 EngDocument599 pages70000769rev.2ecube7 Engrizkiatul brawijayaPas encore d'évaluation
- Patterson - Allergic Diseases 6th EdDocument370 pagesPatterson - Allergic Diseases 6th Edvasile100% (2)
- CV Stoskopf 12 06Document52 pagesCV Stoskopf 12 06shinevoicePas encore d'évaluation
- Emerging and Reemerging Infectious DiseasesDocument25 pagesEmerging and Reemerging Infectious DiseasesNorberto Francisco BaldiPas encore d'évaluation
- Leukemia EssayDocument4 pagesLeukemia EssaydanarajPas encore d'évaluation