Vous aimerez peut-être aussi
- Toksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptDocument51 pagesToksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptRossy OchiePas encore d'évaluation
- Desain Studi Observasional Dalam Farmakoepidemiologi 1 - TugasDocument34 pagesDesain Studi Observasional Dalam Farmakoepidemiologi 1 - Tugasngakan gede sunuartaPas encore d'évaluation
- Farmakoepidemiologi 2018 UmmDocument23 pagesFarmakoepidemiologi 2018 UmmSeptiani Ayu100% (1)
- Post-Marketing Drug SurveillanceDocument123 pagesPost-Marketing Drug SurveillanceRachma DyraPas encore d'évaluation
- Farmasy Farmakoekonomi S1 2021Document67 pagesFarmasy Farmakoekonomi S1 2021MochamadIqbalJaelani100% (1)
- Floating Drug Delivery SystemDocument27 pagesFloating Drug Delivery SystemGANESH KUMAR JELLA100% (1)
- Analisis Pengelolaan Obat Di Puskesmas Kampala Kecamatan Sinjai PDFDocument10 pagesAnalisis Pengelolaan Obat Di Puskesmas Kampala Kecamatan Sinjai PDFPradika Nudya Risalati RachmanPas encore d'évaluation
- Analgetik - Anti Inflamasi - AntipiretikDocument27 pagesAnalgetik - Anti Inflamasi - AntipiretikchrisPas encore d'évaluation
- Pengaruh Kehadiran Apoteker Di ApotekDocument9 pagesPengaruh Kehadiran Apoteker Di ApotekIsra Tri HardiantiPas encore d'évaluation
- Validasi MADocument93 pagesValidasi MADwiPas encore d'évaluation
- Perkembangan Herbal Medicine di IndonesiaDocument47 pagesPerkembangan Herbal Medicine di IndonesiasarinapitupuluPas encore d'évaluation
- Tata Laksana TB MDR Dr. PrayudiDocument58 pagesTata Laksana TB MDR Dr. PrayudiDeaPas encore d'évaluation
- Farmasi Rumah SakitDocument97 pagesFarmasi Rumah SakitkuronohanaPas encore d'évaluation
- Rancangan Penelitian : Research DesignDocument47 pagesRancangan Penelitian : Research DesignrofiPas encore d'évaluation
- Overview Heart Failure: (Hfref, Hfpef)Document37 pagesOverview Heart Failure: (Hfref, Hfpef)Zaras Yudisthira SagaPas encore d'évaluation
- Bioavailability of Topically Administered Ocular DrugsDocument29 pagesBioavailability of Topically Administered Ocular DrugsAry MaringPas encore d'évaluation
- DM - Cardiac-AnaesthesiaDocument19 pagesDM - Cardiac-AnaesthesiaKajori ChakrabortyPas encore d'évaluation
- Pengembangan FormulaDocument95 pagesPengembangan FormulaDikdikPas encore d'évaluation
- Depart. Farmakologi Dan Terapeutik: Universitas Sumatera Utara-MedanDocument19 pagesDepart. Farmakologi Dan Terapeutik: Universitas Sumatera Utara-MedanMasyithah TetaPas encore d'évaluation
- Pemberian Obat Pada AnakDocument19 pagesPemberian Obat Pada AnakMuhamad RockystankiPas encore d'évaluation
- 2011 PK-PD AntibiotikDocument88 pages2011 PK-PD AntibiotikUniatimelindaPas encore d'évaluation
- Pengaruh Kompensasi Terhadap Kepuasan dan Kinerja Karyawan PLN MalangDocument7 pagesPengaruh Kompensasi Terhadap Kepuasan dan Kinerja Karyawan PLN MalangMuhammad Hafif DamanhuriPas encore d'évaluation
- Indonesian Pediatric Endocrinology 4thDocument14 pagesIndonesian Pediatric Endocrinology 4thGendis Ayu ArdiasPas encore d'évaluation
- HotLab Agustus 2019-DikonversiDocument71 pagesHotLab Agustus 2019-DikonversiEndy JuliantoPas encore d'évaluation
- History and Classification of AntibioticsDocument55 pagesHistory and Classification of Antibioticspuspadina ebePas encore d'évaluation
- Penyuluhan Protokol Kesehatan Pencegahan 93693d3aDocument15 pagesPenyuluhan Protokol Kesehatan Pencegahan 93693d3anindi saputriPas encore d'évaluation
- Toksikologi UmumDocument38 pagesToksikologi UmumAndrill VazharyPas encore d'évaluation
- Ion ChannelsDocument21 pagesIon ChannelsAmit SahPas encore d'évaluation
- Metabolit SekunderDocument76 pagesMetabolit SekunderCempaka Kusuma DewiPas encore d'évaluation
- HFA diagnostic algorithm for heart failure with preserved ejection fractionDocument21 pagesHFA diagnostic algorithm for heart failure with preserved ejection fractionCarina UrechePas encore d'évaluation
- Gagal GinjalDocument28 pagesGagal GinjalEnggal HadiPas encore d'évaluation
- Appendisitis: DR Bambang Sugeng Bag. Bedah FK UnissulaDocument33 pagesAppendisitis: DR Bambang Sugeng Bag. Bedah FK UnissulaEsthy Espanyola PelapelaponPas encore d'évaluation
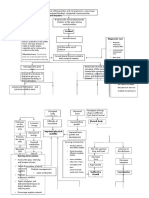
- Pathway - Skoliosis GROUPDocument12 pagesPathway - Skoliosis GROUPAnonymous NZTQVgjaPas encore d'évaluation
- Farmakoterapi Pada LansiaDocument29 pagesFarmakoterapi Pada LansiaPuterinugraha Wanca ApatyaPas encore d'évaluation
- 44 85 1 SMDocument9 pages44 85 1 SMsilvanaanggraeniPas encore d'évaluation
- PERTEMUAN III Desain Sistem Penghantaran Obat BaruDocument51 pagesPERTEMUAN III Desain Sistem Penghantaran Obat BaruSari Ramadhani100% (1)
- RCTS Clinical Trials RandomizationDocument35 pagesRCTS Clinical Trials RandomizationFatt ZakiPas encore d'évaluation
- 01 C & D Latar Belakang GPPDocument38 pages01 C & D Latar Belakang GPPPrisma TridaPas encore d'évaluation
- Progress Project Mingguan Rev01Document62 pagesProgress Project Mingguan Rev01Vita Monica SariPas encore d'évaluation
- ADMEDocument21 pagesADMEanisaPas encore d'évaluation
- Pharmaco VigilanceDocument31 pagesPharmaco VigilanceRasika NatuPas encore d'évaluation
- Pharmacovigilance FinalDocument71 pagesPharmacovigilance Finalabdullah2020100% (1)
- Drug Discovery and Development: From Bench to BedsideDocument23 pagesDrug Discovery and Development: From Bench to BedsideAhmed HamarnehPas encore d'évaluation
- PharmacovigilanceDocument31 pagesPharmacovigilanceapi-381097683% (6)
- PVDocument58 pagesPVVikram MishraPas encore d'évaluation
- 1.1 Definition, Origin, Scope, Aims and Applications of Pharmacoepideomology - Pharmacoepidemiology and PharmacoeconomicsDocument11 pages1.1 Definition, Origin, Scope, Aims and Applications of Pharmacoepideomology - Pharmacoepidemiology and Pharmacoeconomicskauser.erum11Pas encore d'évaluation
- SEMINAR - 7 (Pharmacoepidemilogy)Document69 pagesSEMINAR - 7 (Pharmacoepidemilogy)LathaVijendraPas encore d'évaluation
- Pharmacoepidemiology 9Document29 pagesPharmacoepidemiology 9Ani RahayuPas encore d'évaluation
- Sistem PelaporanDocument21 pagesSistem PelaporanRifat SaufiPas encore d'évaluation
- PHARMACOVIGILANCE - Std-Ed 1-22Document54 pagesPHARMACOVIGILANCE - Std-Ed 1-22cellinapratiwiPas encore d'évaluation
- 01 - Spontaneous Reporting Quality of The ReportDocument27 pages01 - Spontaneous Reporting Quality of The ReportMaya DwiyantiPas encore d'évaluation
- Clinical Trial Gadavala SarahDocument60 pagesClinical Trial Gadavala SarahSejal khuman100% (1)
- Phases of Clinical TrialsDocument30 pagesPhases of Clinical TrialsMahum SohailPas encore d'évaluation
- Drug Development and EvaluationDocument25 pagesDrug Development and EvaluationArlises SinagaPas encore d'évaluation
- Post Marketing SurveillanceDocument15 pagesPost Marketing SurveillanceSundar Karuna100% (1)
- Introduction to PharmacovigillanceDocument93 pagesIntroduction to Pharmacovigillancefunnymemesworld2023Pas encore d'évaluation
- Historyofclinicaltrials 130917044916 Phpapp02Document55 pagesHistoryofclinicaltrials 130917044916 Phpapp02Akshay SablePas encore d'évaluation
- ADRpptDocument35 pagesADRpptRobert Selvin MPas encore d'évaluation
- Rational Use of Drugs and Evidence Based Medicine: Department of Pharmacology NEIGRIHMS, ShillongDocument31 pagesRational Use of Drugs and Evidence Based Medicine: Department of Pharmacology NEIGRIHMS, Shillongdbrahma100% (1)
- Pharmacoepidemiology Drug StudiesDocument61 pagesPharmacoepidemiology Drug StudiesDrvinay Goud50% (2)
- Curriculum Vitae: Personal InformationDocument2 pagesCurriculum Vitae: Personal InformationArif Muhammad YunanPas encore d'évaluation
- Gela-Malta (Cost Estimate) Rev 2 3 PDFDocument21 pagesGela-Malta (Cost Estimate) Rev 2 3 PDFArif Muhammad Yunan100% (1)
- Group 5Document13 pagesGroup 5Arif Muhammad YunanPas encore d'évaluation
- Cover 2013 Keatas AkDocument1 pageCover 2013 Keatas AkArif Muhammad YunanPas encore d'évaluation
- PEGS CatalogDocument88 pagesPEGS CatalogMPas encore d'évaluation
- AirDocument218 pagesAirPankaj Wamanrao Bomble0% (1)
- Formulary Book - Hajer (1) Final To Print1 MOH HospitalDocument115 pagesFormulary Book - Hajer (1) Final To Print1 MOH HospitalspiderPas encore d'évaluation
- Persuasive Essay - 2nd Draft 2Document11 pagesPersuasive Essay - 2nd Draft 2api-301813354Pas encore d'évaluation
- Pharmacology MnemonicsDocument19 pagesPharmacology MnemonicsAl-nazer Azer Al100% (5)
- ADHD: Clinical Practice Guideline For The Diagnosis, Evaluation, and TreatmentDocument18 pagesADHD: Clinical Practice Guideline For The Diagnosis, Evaluation, and TreatmentBen CulpepperPas encore d'évaluation
- 2015 07 10 Pharma Distribution RomaniaDocument2 pages2015 07 10 Pharma Distribution RomaniaVanillaheroinePas encore d'évaluation
- Case Study Notes - CSIDocument39 pagesCase Study Notes - CSIRinder SidhuPas encore d'évaluation
- Pharmacovigilance EnglishDocument4 pagesPharmacovigilance EnglishImmad AlviPas encore d'évaluation
- Cures, Health & Wellbeing PDFDocument1 741 pagesCures, Health & Wellbeing PDFkitty katPas encore d'évaluation
- Critical overview of India's patent lawDocument21 pagesCritical overview of India's patent lawNishant Bhaskaran100% (2)
- A Brief Note On Plants of Medicinal Importance To LivestockDocument84 pagesA Brief Note On Plants of Medicinal Importance To LivestockSunil100% (1)
- IPL - Roma Drug vs. RTCDocument2 pagesIPL - Roma Drug vs. RTCEly R. BarrettoPas encore d'évaluation
- Pharmacology and Therapeutics in Dentistry: Periodontology 2000Document2 pagesPharmacology and Therapeutics in Dentistry: Periodontology 2000BimalKrishnaPas encore d'évaluation
- Week 1 DavidsonX D001x Medicinal Chemistry Weekly SummaryDocument28 pagesWeek 1 DavidsonX D001x Medicinal Chemistry Weekly SummaryAna Laura PérezPas encore d'évaluation
- Biomems As A Tool To Decifer The Shortcomings of Pharmaceutical Analysis and Importance in Patient Self CareDocument2 pagesBiomems As A Tool To Decifer The Shortcomings of Pharmaceutical Analysis and Importance in Patient Self CareInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Kantalohahaematinicrs016gdg 121228221817 Phpapp02Document166 pagesKantalohahaematinicrs016gdg 121228221817 Phpapp02Vaidya NurPas encore d'évaluation
- 08 Drug ProfileDocument2 pages08 Drug ProfilekurutalaPas encore d'évaluation
- Regulatory Perspective - Yukio HiyamaDocument32 pagesRegulatory Perspective - Yukio Hiyamasksingh82Pas encore d'évaluation
- Elcam-3D Long-Duration SQ Patch PumpDocument1 pageElcam-3D Long-Duration SQ Patch PumpgshgssgPas encore d'évaluation
- Pharmacist Role in Health Care SystemDocument8 pagesPharmacist Role in Health Care SystemLoo Soo WeiPas encore d'évaluation
- Postapproval CMC ChangesDocument12 pagesPostapproval CMC ChangesSondell100% (1)
- VP Global Marketing Pharmaceuticals Biotech Industry in New York Metropolitan Resume Renate ReissDocument3 pagesVP Global Marketing Pharmaceuticals Biotech Industry in New York Metropolitan Resume Renate ReissRenate ReissPas encore d'évaluation
- MRCF Guidelines DraftDocument32 pagesMRCF Guidelines DraftvrtzioPas encore d'évaluation
- Fast Dissolving Tablets: A Novel Approch To Drug Delivery - A ReviewDocument10 pagesFast Dissolving Tablets: A Novel Approch To Drug Delivery - A ReviewNova Lya SipahutarPas encore d'évaluation
- FAQ Residual SolventDocument4 pagesFAQ Residual SolventDilla Wulan NingrumPas encore d'évaluation
- Michelle Garner ResumeDocument2 pagesMichelle Garner Resumetuc30218Pas encore d'évaluation
- HOBERMAN 2005 Testosterone Dreams PDFDocument390 pagesHOBERMAN 2005 Testosterone Dreams PDFLucasTramontanoPas encore d'évaluation
- Anti-Microbial Activity of Cassia Tora Leaves and Stems Crude ExtractDocument4 pagesAnti-Microbial Activity of Cassia Tora Leaves and Stems Crude ExtractHelixPas encore d'évaluation
- Cure For CancerDocument6 pagesCure For CancerSimanjuntak Sitombuk MarganaPas encore d'évaluation