Vous aimerez peut-être aussi
- Heart FailureDocument22 pagesHeart FailureYoussef MansourPas encore d'évaluation
- Heart Failure CardiologyDocument25 pagesHeart Failure CardiologyPAN FRAGGERPas encore d'évaluation
- FINAL CARDIOMYOPATHIESDocument53 pagesFINAL CARDIOMYOPATHIESAmosPas encore d'évaluation
- Essential Guide to Heart FailureDocument59 pagesEssential Guide to Heart FailureMahesh RathnayakePas encore d'évaluation
- Cardiac Failure Diagnosis and TreatmentDocument5 pagesCardiac Failure Diagnosis and TreatmentMatyie SmkasPas encore d'évaluation
- Cor Pulmonale: Definition, Causes, Symptoms & TreatmentDocument31 pagesCor Pulmonale: Definition, Causes, Symptoms & TreatmentAnjela BaidyaPas encore d'évaluation
- Heart To HeartDocument110 pagesHeart To HeartmahyorwaPas encore d'évaluation
- Valvular Heart DseDocument8 pagesValvular Heart DseJane Pineda CuraPas encore d'évaluation
- Congestive Heart FailureDocument28 pagesCongestive Heart Failuresarguss1480% (5)
- Cardio Notes, Heart FailureDocument17 pagesCardio Notes, Heart FailureJoy DunwanPas encore d'évaluation
- Kuliah Gagal JantungDocument47 pagesKuliah Gagal JantungRangga Alam VaneoPas encore d'évaluation
- Congestive Heart FailureDocument25 pagesCongestive Heart FailuredevianiamalinaPas encore d'évaluation
- Congestive Heart FailureDocument14 pagesCongestive Heart Failurelolo0880Pas encore d'évaluation
- HEART FAILURE: CAUSES, DIAGNOSIS AND TREATMENTDocument48 pagesHEART FAILURE: CAUSES, DIAGNOSIS AND TREATMENTAlbert SitepuPas encore d'évaluation
- Seminar On Heart Failure: Presented by Neethu.MDocument59 pagesSeminar On Heart Failure: Presented by Neethu.MNeethu JayasankarPas encore d'évaluation
- Heart FaiilureDocument8 pagesHeart Faiilureagar agarPas encore d'évaluation
- 8A - Heart FailureDocument114 pages8A - Heart FailureShahpoor Ahmad ShirzadaPas encore d'évaluation
- CHFDocument35 pagesCHFMarione GimenezPas encore d'évaluation
- Cardiovascular DisordersDocument38 pagesCardiovascular Disordersmark100% (4)
- Pulm HTNDocument62 pagesPulm HTNJonathan LongPas encore d'évaluation
- Heart FailureDocument10 pagesHeart Failureurmila prajapatiPas encore d'évaluation
- Chinonye Ekeocha, Tazleem Khan, Ogechi Ekeocha August 23, 2010 Jackson Park Hospital Internal Medicine Core ClerkshipDocument31 pagesChinonye Ekeocha, Tazleem Khan, Ogechi Ekeocha August 23, 2010 Jackson Park Hospital Internal Medicine Core ClerkshipsgolbariPas encore d'évaluation
- CHFDocument45 pagesCHFAry 01Pas encore d'évaluation
- Congestive Hearth FailureDocument6 pagesCongestive Hearth FailureIqbal BatubaraPas encore d'évaluation
- Heart Failure: Understanding the Definition, Causes, Symptoms and TreatmentDocument48 pagesHeart Failure: Understanding the Definition, Causes, Symptoms and TreatmentSanjay SathasevanPas encore d'évaluation
- Heart Failure: Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanDocument42 pagesHeart Failure: Departemen Kardiologi FK USU RSUP. H. Adam Malik Medanbilli lisanuddinPas encore d'évaluation
- Gagal JantungDocument54 pagesGagal JantungMiftahul IfahPas encore d'évaluation
- Congestive heart failure fileDocument31 pagesCongestive heart failure fileAbas AhmedPas encore d'évaluation
- Shock: Ibrahim Ali & Winfred C. ParnellDocument30 pagesShock: Ibrahim Ali & Winfred C. ParnellsgolbariPas encore d'évaluation
- ACUTE DECOMPENSATED HEART FAILUREDocument71 pagesACUTE DECOMPENSATED HEART FAILUREVivek Anandan100% (1)
- Congestive Cardiac FailureDocument38 pagesCongestive Cardiac FailureSalman KhanPas encore d'évaluation
- Cardiovascular Diseases: DR Raveendra K.R Assistant Professor Department of Medicine BMC BangaloreDocument34 pagesCardiovascular Diseases: DR Raveendra K.R Assistant Professor Department of Medicine BMC BangalorerameshbmcPas encore d'évaluation
- Cardaic ArrestDocument17 pagesCardaic ArrestM Farhad KhaniPas encore d'évaluation
- Heart Failure: Low Output HF High Output HFDocument7 pagesHeart Failure: Low Output HF High Output HFJake BurrPas encore d'évaluation
- CHFDocument35 pagesCHFirenePas encore d'évaluation
- Heart Failure: DR Kaem Shir AliDocument24 pagesHeart Failure: DR Kaem Shir AliMwanja MosesPas encore d'évaluation
- Heart Failure & Cardiac Arrest: Rony YuliwansyahDocument92 pagesHeart Failure & Cardiac Arrest: Rony YuliwansyahSasha ManoPas encore d'évaluation
- Heart FailureDocument94 pagesHeart FailureAnusha Verghese100% (1)
- CHFDocument22 pagesCHFshazia kaziPas encore d'évaluation
- Comprehensive Study of Beta BlockersDocument40 pagesComprehensive Study of Beta Blockersapi-369859880% (5)
- Congestive Heart Failure: Mulualem W.MD Dmu, Department of Internal Medicine For Ho StudentsDocument27 pagesCongestive Heart Failure: Mulualem W.MD Dmu, Department of Internal Medicine For Ho Studentsmuluneh birhanePas encore d'évaluation
- Clinical Aspect of Heart FailureDocument67 pagesClinical Aspect of Heart FailureAri Bandana TasrifPas encore d'évaluation
- Congestive Heart Failure ReportDocument6 pagesCongestive Heart Failure ReportSunshine_Bacla_4275100% (1)
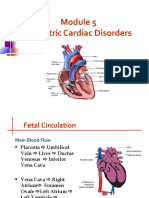
- Pediatric Cardiac Disorders: Fetal Circulation and Congestive Heart FailureDocument62 pagesPediatric Cardiac Disorders: Fetal Circulation and Congestive Heart FailureMarie Queenly Pagaran100% (1)
- Right Sided Heart Failure Case 4.2Document4 pagesRight Sided Heart Failure Case 4.2Athari AdityaPas encore d'évaluation
- Pathophysiology of Congestive Heart Failure: Cardiovascular SystemDocument3 pagesPathophysiology of Congestive Heart Failure: Cardiovascular Systembanyenye25Pas encore d'évaluation
- Lec 3 Heart FailureDocument25 pagesLec 3 Heart FailureDelete AccountPas encore d'évaluation
- Cardiac Failure & Myocardial Infarction GuideDocument6 pagesCardiac Failure & Myocardial Infarction GuideDaniel GeduquioPas encore d'évaluation
- Cardiogenic ShockDocument27 pagesCardiogenic ShockIgor StefanetPas encore d'évaluation
- K7 - Penyakit Jantung Katub-ANNDocument38 pagesK7 - Penyakit Jantung Katub-ANNXeniel AlastairPas encore d'évaluation
- Heart Failure and ShockDocument34 pagesHeart Failure and Shockfrenee aradanasPas encore d'évaluation
- Cardiac Failure: Dr. Abdul Ghani WaseemDocument33 pagesCardiac Failure: Dr. Abdul Ghani WaseemFarwaPas encore d'évaluation
- Heart Failure: Kalaiselvan OtDocument46 pagesHeart Failure: Kalaiselvan Otplayme_nowPas encore d'évaluation
- Rheumatic Fever and Rheumatic CarditisDocument8 pagesRheumatic Fever and Rheumatic CarditisDyanne Tan DabuPas encore d'évaluation
- Braunwald Lecture Series #2Document33 pagesBraunwald Lecture Series #2usfcards100% (2)
- Hypertensive Crisis: Megat Mohd Azman Bin AdzmiDocument34 pagesHypertensive Crisis: Megat Mohd Azman Bin AdzmiMegat Mohd Azman AdzmiPas encore d'évaluation
- Cardiac Heart Failure Guide: Causes, Symptoms & Nursing CareDocument43 pagesCardiac Heart Failure Guide: Causes, Symptoms & Nursing CareCindy DeliaPas encore d'évaluation
- Pharmacotherapeutic Management of Cardiovascular Disease Complications: A Textbook for Medical StudentsD'EverandPharmacotherapeutic Management of Cardiovascular Disease Complications: A Textbook for Medical StudentsPas encore d'évaluation
- Pathophysiology, Risk Factors, and Management of Chronic Heart FailureD'EverandPathophysiology, Risk Factors, and Management of Chronic Heart FailureRam B. SinghPas encore d'évaluation
- 20 Items Emergency RawDocument6 pages20 Items Emergency RawGodfrey FrancoPas encore d'évaluation
- 20 Items Emrgency Nursing ReviewDocument4 pages20 Items Emrgency Nursing ReviewGodfrey FrancoPas encore d'évaluation
- NLE Poisons and AntidotesDocument2 pagesNLE Poisons and AntidotesGodfrey Franco100% (1)
- Funda BulletsDocument183 pagesFunda BulletsGodfrey FrancoPas encore d'évaluation
- Professional Adjustment and Nursing JurisprudenceDocument65 pagesProfessional Adjustment and Nursing JurisprudenceJAY LAPAZ ANDRES, RN, BSN, MAN (C), MAEd.. (C)100% (2)
- Antimalarial, Antiprotozoal, and Antihelmintic AgentsDocument37 pagesAntimalarial, Antiprotozoal, and Antihelmintic AgentsLady Mae RamosPas encore d'évaluation
- PharmacologyDocument33 pagesPharmacologyFreeNursingNotes90% (67)
- Chapter 2Document9 pagesChapter 2Godfrey FrancoPas encore d'évaluation
- PharmacologyDocument33 pagesPharmacologyFreeNursingNotes90% (67)
- Aged Care SpecializationDocument2 pagesAged Care SpecializationGodfrey FrancoPas encore d'évaluation
- QuestionsDocument2 pagesQuestionsGodfrey FrancoPas encore d'évaluation
- INSTRUCTIONAL DESIGN Aged Care SpeializationDocument8 pagesINSTRUCTIONAL DESIGN Aged Care SpeializationGodfrey FrancoPas encore d'évaluation
- Future Directions : Understanding Cultural Diversity and Surviving Life AbroadDocument24 pagesFuture Directions : Understanding Cultural Diversity and Surviving Life AbroadGodfrey FrancoPas encore d'évaluation
- Medical Surgical Nursing ConceptsDocument139 pagesMedical Surgical Nursing ConceptsGodfrey FrancoPas encore d'évaluation
- Pharmacology Made Insanely Easy PowerPointDocument42 pagesPharmacology Made Insanely Easy PowerPointBetsy Brown Byersmith82% (22)
- Culture Care and DiversityDocument11 pagesCulture Care and DiversityGodfrey Franco0% (1)
- Inflammatory Conditions of HeartDocument28 pagesInflammatory Conditions of HeartGodfrey Franco100% (1)
- Geriatric Nursing Terms and ConceptsDocument53 pagesGeriatric Nursing Terms and ConceptsGodfrey FrancoPas encore d'évaluation
- Valvular Heart Disease Medical Surgical NursingDocument75 pagesValvular Heart Disease Medical Surgical NursingGodfrey Franco88% (8)
- Nursing Care of Patients With Skin DisordersDocument69 pagesNursing Care of Patients With Skin DisordersGodfrey FrancoPas encore d'évaluation
- Nursing ResearchDocument37 pagesNursing ResearchGodfrey FrancoPas encore d'évaluation
- Circulatory SystemDocument19 pagesCirculatory SystemGodfrey FrancoPas encore d'évaluation
- COMPETENCY-BASED CURRICULUM DEVELOPMENT - Paper2Document19 pagesCOMPETENCY-BASED CURRICULUM DEVELOPMENT - Paper2108balajiPas encore d'évaluation
- Nursing Leadership and ManagementDocument43 pagesNursing Leadership and Managementbajaoc95% (22)
- Gastrointestinal IntubationsDocument48 pagesGastrointestinal IntubationsGodfrey FrancoPas encore d'évaluation
- Introduction To Nursing Research in An Evidence-Based Practice EnvironmentDocument10 pagesIntroduction To Nursing Research in An Evidence-Based Practice EnvironmentpamgelPas encore d'évaluation
- Professional AdjustmentDocument140 pagesProfessional AdjustmentGodfrey FrancoPas encore d'évaluation
- Obstructive Sleep Apnea - Pulmo LectureDocument16 pagesObstructive Sleep Apnea - Pulmo LecturemandrakesMD0% (1)
- Monitoring Your Glucose LevelDocument4 pagesMonitoring Your Glucose LevelSarah OmarPas encore d'évaluation
- The digestive system explainedDocument4 pagesThe digestive system explainedStephanie ZammitPas encore d'évaluation
- Anatomy and PhysiologyDocument5 pagesAnatomy and Physiologyjohnbech07Pas encore d'évaluation
- Pediatric Obesity AlgorithmDocument92 pagesPediatric Obesity AlgorithmAnonymous wuXj8ns9Pas encore d'évaluation
- Obesity What Is Obesity?Document12 pagesObesity What Is Obesity?TABIBI11Pas encore d'évaluation
- Basic Medial Science of The Kidney: The Scientific Basis of Clinical Disease, Marc Imhotep Cray, M.D.Document193 pagesBasic Medial Science of The Kidney: The Scientific Basis of Clinical Disease, Marc Imhotep Cray, M.D.Marc Imhotep Cray, M.D.100% (3)
- Metabolic Interreationships - MED PDFDocument63 pagesMetabolic Interreationships - MED PDFDr.Ghazala Kaukab RajaPas encore d'évaluation
- Excess Fat Intake Diagnosis GuideDocument2 pagesExcess Fat Intake Diagnosis GuideDede KecilPas encore d'évaluation
- Management Nutrisi Pada Stroke Akut DR Mursyid FinalDocument31 pagesManagement Nutrisi Pada Stroke Akut DR Mursyid Finalkanes eisaPas encore d'évaluation
- Gestational Diabetes MellitusDocument25 pagesGestational Diabetes MellitusMazlina MaidinPas encore d'évaluation
- Soft Gluten Free Vegan Bread Recipe - Easy & Delicious!Document49 pagesSoft Gluten Free Vegan Bread Recipe - Easy & Delicious!jamesPas encore d'évaluation
- Pemeriksaan AbdomenDocument212 pagesPemeriksaan Abdomentamara hanna bocanPas encore d'évaluation
- Top 10 Health Benefits of Okra (Lady's Finger)Document4 pagesTop 10 Health Benefits of Okra (Lady's Finger)ozoemena29Pas encore d'évaluation
- Thesis T3003 PDFDocument99 pagesThesis T3003 PDFNor HidayahPas encore d'évaluation
- Case Study ObesityDocument2 pagesCase Study ObesityPaolo Alshu PacresPas encore d'évaluation
- Dietary Analysis ReportDocument8 pagesDietary Analysis Reportapi-542955719Pas encore d'évaluation
- JCC Membership Packages and Benefits for Families and IndividualsDocument2 pagesJCC Membership Packages and Benefits for Families and IndividualsDiane YangPas encore d'évaluation
- Epsom SaltDocument9 pagesEpsom SaltbonifacesilveiraPas encore d'évaluation
- Cushing SyndromeDocument2 pagesCushing SyndromeKesyaPas encore d'évaluation
- Umftgm 2017 MarissiensisDocument148 pagesUmftgm 2017 MarissiensisAdriana VillarrealPas encore d'évaluation
- A little bit of what you fancy and diet defianceDocument3 pagesA little bit of what you fancy and diet defiancealwinalexanderPas encore d'évaluation
- The Role of Diet in Cancer Prevention and Chemotherapy EfficacyDocument25 pagesThe Role of Diet in Cancer Prevention and Chemotherapy EfficacyXabier EzkerraPas encore d'évaluation
- Insuline IndexDocument28 pagesInsuline IndexcasaberkanePas encore d'évaluation
- TT Bootcamp Games ManualDocument33 pagesTT Bootcamp Games Manualtano47Pas encore d'évaluation
- Latihan Simak 4Document6 pagesLatihan Simak 4Fendy Eko HariyantoPas encore d'évaluation
- Guided Project 4-2Document2 pagesGuided Project 4-2MichaelPas encore d'évaluation
- How ultrasound diagnosed gallstonesDocument25 pagesHow ultrasound diagnosed gallstonesJulie Mae Asuncion RigosPas encore d'évaluation
- Gencardio BmiDocument11 pagesGencardio BmiGabriel CallupePas encore d'évaluation
- CCEA - AS - Health and Social Care - Socio Economic Factors - UNIT 3Document23 pagesCCEA - AS - Health and Social Care - Socio Economic Factors - UNIT 3rubaalsirahmedPas encore d'évaluation