Vous aimerez peut-être aussi
- CIC Prep 9 19 13Document28 pagesCIC Prep 9 19 13ksibinpaulPas encore d'évaluation
- Cyberoam Next-Gen Security for EnterprisesDocument7 pagesCyberoam Next-Gen Security for EnterprisesksibinpaulPas encore d'évaluation
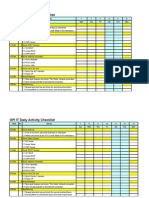
- IT Daily Activities ChecklistDocument5 pagesIT Daily Activities ChecklistksibinpaulPas encore d'évaluation
- How To - Allow Secured Internet Access To Guest UsersDocument10 pagesHow To - Allow Secured Internet Access To Guest UsersksibinpaulPas encore d'évaluation
- Ax Installation GuideDocument198 pagesAx Installation GuideksibinpaulPas encore d'évaluation
- Microsoft Dynamics AX 2012 Licensing Guide July 2012 Customer EditionDocument23 pagesMicrosoft Dynamics AX 2012 Licensing Guide July 2012 Customer EditionksibinpaulPas encore d'évaluation
- Sample AX2012 ReportsDocument27 pagesSample AX2012 ReportsksibinpaulPas encore d'évaluation
- Itil: The Basics: Valerie Arraj, Compliance Process Partners LLCDocument5 pagesItil: The Basics: Valerie Arraj, Compliance Process Partners LLCdmr1982Pas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5783)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Carroll University Hospital PDFDocument0 pageCarroll University Hospital PDFSteve BlubaughPas encore d'évaluation
- Emergency Care For Patients With Hemophilia FINALDocument28 pagesEmergency Care For Patients With Hemophilia FINALebillPas encore d'évaluation
- Challenging Concepts in INTERVENTIONAL RADIOLOGY 1st EditionDocument363 pagesChallenging Concepts in INTERVENTIONAL RADIOLOGY 1st EditionHisham Elkilaney100% (1)
- Panre and Pance Review Cardiovascular IIDocument26 pagesPanre and Pance Review Cardiovascular IIThe Physician Assistant Life100% (1)
- MemonDocument5 pagesMemonvamsi NathPas encore d'évaluation
- Stepladder Plating Following Lower Subapical and Geniop - 2022 - Advances in OraDocument2 pagesStepladder Plating Following Lower Subapical and Geniop - 2022 - Advances in OraГне ДзжPas encore d'évaluation
- Human Body Systems - Digestive and Excretory 1920Document18 pagesHuman Body Systems - Digestive and Excretory 1920api-409777377Pas encore d'évaluation
- Improving vision through cataract procedures and YAG capsulotomyDocument9 pagesImproving vision through cataract procedures and YAG capsulotomyBplo CaloocanPas encore d'évaluation
- NSG 700 - Organ TranspantDocument30 pagesNSG 700 - Organ TranspantJellou MacPas encore d'évaluation
- (Mebooksfree Net) Ric&vas&tra&ras&tai&3rd PDFDocument416 pages(Mebooksfree Net) Ric&vas&tra&ras&tai&3rd PDFAlexandru ChiriacPas encore d'évaluation
- Case Studies - MIC3002Document28 pagesCase Studies - MIC300217206404 STUDENTPas encore d'évaluation
- Dystocia SOGCDocument16 pagesDystocia SOGCAdhitia NugrahantoPas encore d'évaluation
- Improving Physical Mobility Through Nursing InterventionsDocument2 pagesImproving Physical Mobility Through Nursing InterventionsPrincess Averin Navarro50% (2)
- Literature ReviewDocument3 pagesLiterature Reviewapi-534368223Pas encore d'évaluation
- G-CFA Instructor Tab 6-2 Handout 2 Sample Adequate Nursing Care Plan-R6Document2 pagesG-CFA Instructor Tab 6-2 Handout 2 Sample Adequate Nursing Care Plan-R6SriMathi Kasi Malini ArmugamPas encore d'évaluation
- Lower Respiratory Disorders Part 1Document70 pagesLower Respiratory Disorders Part 1Joseph Krafft100% (1)
- Implant Surgery Complications - Etiology and TreatmentDocument10 pagesImplant Surgery Complications - Etiology and TreatmentStephanie JaramilloPas encore d'évaluation
- CV Disease Drug StudyDocument11 pagesCV Disease Drug StudyMaria Francheska OsiPas encore d'évaluation
- 6 Pack Sept 2013-OEC-Shock-Chapter 10 - NSPDocument23 pages6 Pack Sept 2013-OEC-Shock-Chapter 10 - NSPDonavon GaudettePas encore d'évaluation
- Referral Form TemplateDocument1 pageReferral Form TemplateVMPas encore d'évaluation
- TLE Beauty Care Pretest Grade910Document4 pagesTLE Beauty Care Pretest Grade910KENT REEVE ROSALPas encore d'évaluation
- Laporan Faal Respi 2021 - Kenni KenedyDocument25 pagesLaporan Faal Respi 2021 - Kenni Kenedykenni kenedyPas encore d'évaluation
- PTSHH0119.006.2015 The Importance of Contact Times For DisinfectantsDocument2 pagesPTSHH0119.006.2015 The Importance of Contact Times For DisinfectantsbluemojoPas encore d'évaluation
- TMC213. Bacalso - Bstm2a.module 2, L3Document7 pagesTMC213. Bacalso - Bstm2a.module 2, L3John Ariel Labnao GelbolingoPas encore d'évaluation
- Diabetic Ketoacidosis - Anand Singh BrarDocument5 pagesDiabetic Ketoacidosis - Anand Singh BrarAnand Singh BrarPas encore d'évaluation
- PracticeExam 2 AnsDocument51 pagesPracticeExam 2 AnsBehrouz YariPas encore d'évaluation
- Continuous Renal Replacement TherapyDocument38 pagesContinuous Renal Replacement Therapyanju rachel josePas encore d'évaluation
- Compiledendo PerioDocument112 pagesCompiledendo PerioAvner TolentinoPas encore d'évaluation
- Child with noisy breathing and drooling has bronchiolitisDocument3 pagesChild with noisy breathing and drooling has bronchiolitissaudPas encore d'évaluation
- Evidence-Based Medicine: David L. SackettDocument3 pagesEvidence-Based Medicine: David L. SackettNicolas MarinPas encore d'évaluation