Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- (Lib-Ebooks Com) 050420202258 PDFDocument3 395 pages(Lib-Ebooks Com) 050420202258 PDFruchikaPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- (PDFmedbook - Blogspot.com) Andrea Ann Borchers Ed. Handbook of Signs Symptoms LWW Wolters KluwerDocument919 pages(PDFmedbook - Blogspot.com) Andrea Ann Borchers Ed. Handbook of Signs Symptoms LWW Wolters KluwerKatherynPas encore d'évaluation
- Abdominal Wall HerniaDocument100 pagesAbdominal Wall Herniaintandiahningrum100% (1)
- EHS Groin Hernia ClassificationDocument4 pagesEHS Groin Hernia ClassificationbogdanotiPas encore d'évaluation
- Gastrointestinal Disorders PnleDocument23 pagesGastrointestinal Disorders Pnledelieup02100% (2)
- Indirect Inguinal HerniaDocument54 pagesIndirect Inguinal HerniaYlamher Bufi Imperial100% (1)
- HerniaDocument41 pagesHerniashobharamkrishna67% (3)
- Herniorrhaphy Procedure Repairs Hernia Through SuturesDocument2 pagesHerniorrhaphy Procedure Repairs Hernia Through SuturesSheldon Deypalubos Jr.Pas encore d'évaluation
- Acute Appendicitis Signs, Symptoms & DiagnosisDocument70 pagesAcute Appendicitis Signs, Symptoms & DiagnosisTimbur IgorPas encore d'évaluation
- Bengt Novik,, Gabriel Sandblom,, Christoph Ansorge,, Anders ThorellDocument15 pagesBengt Novik,, Gabriel Sandblom,, Christoph Ansorge,, Anders ThorellAndric Perez-OrtizPas encore d'évaluation
- Hernias Case PresentationDocument46 pagesHernias Case Presentationraxym17Pas encore d'évaluation
- TOP DIAGNOSIS FOR SURGERY AND EMERGENCY DEPARTMENTDocument4 pagesTOP DIAGNOSIS FOR SURGERY AND EMERGENCY DEPARTMENTfebrikurniasariPas encore d'évaluation
- Hernia and LutzDocument4 pagesHernia and LutzDrew CabigaoPas encore d'évaluation
- Cholecystectomy GuideDocument4 pagesCholecystectomy GuideKim Glaidyl BontuyanPas encore d'évaluation
- S1 Revision by Hania KhanDocument87 pagesS1 Revision by Hania KhanZoha AzizPas encore d'évaluation
- Capacity CaseDocument36 pagesCapacity Casejohnmia20Pas encore d'évaluation
- Pemicu 4 Git Aldi FDocument93 pagesPemicu 4 Git Aldi Faldi firdausPas encore d'évaluation
- Lower Abdominal PainDocument13 pagesLower Abdominal PainhomjungPas encore d'évaluation
- Fellowship in Ivf Training Programme Fellowship in Ivf Training ProgrammeDocument15 pagesFellowship in Ivf Training Programme Fellowship in Ivf Training ProgrammerebarrycosmeticsPas encore d'évaluation
- The Pediatric Surgery Milestone Project: A Joint Initiative ofDocument27 pagesThe Pediatric Surgery Milestone Project: A Joint Initiative ofandreshuertaPas encore d'évaluation
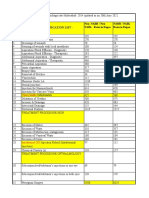
- CGHS package rates Hyderabad updated June 2022Document60 pagesCGHS package rates Hyderabad updated June 2022Pradeep PaswanPas encore d'évaluation
- Hanny Fuzi Jurnal DR BambangDocument30 pagesHanny Fuzi Jurnal DR Bambangfahryzal_notePas encore d'évaluation
- ICD-10 Diagnoses for Bacterial, Viral and Parasitic Meningitis, Encephalitis, and SepsisDocument260 pagesICD-10 Diagnoses for Bacterial, Viral and Parasitic Meningitis, Encephalitis, and SepsisAndreasAndokoPas encore d'évaluation
- Sample: Pediatric Hernia Inguinal and Femoral RepairDocument8 pagesSample: Pediatric Hernia Inguinal and Femoral RepairSamuel Sebastian SirapanjiPas encore d'évaluation
- Nurse QuestionDocument20 pagesNurse QuestionAlenFluxPas encore d'évaluation
- Pediatric HerniaDocument4 pagesPediatric HerniaRudi haris munandar0% (1)
- Anoto Clinica y QX en HerniasDocument7 pagesAnoto Clinica y QX en HerniasDanielaPas encore d'évaluation
- HerniaDocument37 pagesHerniaNoreen Hannah GabrielPas encore d'évaluation
- Hernia ClassificationDocument15 pagesHernia ClassificationAgung SetiawanPas encore d'évaluation
- Test - Surgery Book MCQs - Final Exam - QuizletDocument158 pagesTest - Surgery Book MCQs - Final Exam - Quizlety SPas encore d'évaluation