Vous aimerez peut-être aussi
- Chapter 1Document26 pagesChapter 1Reigner Jay B. Escartin100% (1)
- Lesson 5 The UrineDocument44 pagesLesson 5 The UrineFaith TambongPas encore d'évaluation
- The Nematodes Nema: Thread, Oides: FormDocument20 pagesThe Nematodes Nema: Thread, Oides: FormChandra Adie100% (1)
- Unit 4Document117 pagesUnit 4Soc Sci0% (1)
- Am Positive & Gram Negative Cocci InfectionsDocument33 pagesAm Positive & Gram Negative Cocci InfectionsRebeka Costantina Weriditi0% (1)
- Lesson 1 History of Medical Technology or The Clinical Laboratory Science ProfessionDocument4 pagesLesson 1 History of Medical Technology or The Clinical Laboratory Science ProfessionGianneCarloGomedPas encore d'évaluation
- Introduction of ParasitologyDocument47 pagesIntroduction of ParasitologyNadiya Afifah100% (1)
- Vibrio (Comma-Shaped or Curved Bacillus)Document10 pagesVibrio (Comma-Shaped or Curved Bacillus)Ira ElizagaPas encore d'évaluation
- Introduction To Pathology: DR AL Munawir, Ph.D. Lab. Patologi Anatomi FK Universitas JemberDocument30 pagesIntroduction To Pathology: DR AL Munawir, Ph.D. Lab. Patologi Anatomi FK Universitas JemberEvans Hansen100% (1)
- TB AFB Smear Microscopy TrainerNotes PDFDocument67 pagesTB AFB Smear Microscopy TrainerNotes PDFShiro AsamiPas encore d'évaluation
- Lecture 4. Synovial Fluid CompositionDocument33 pagesLecture 4. Synovial Fluid CompositionDr. AyshaPas encore d'évaluation
- PST RevDocument31 pagesPST Revjada germainePas encore d'évaluation
- Lab. Activity MycologyDocument61 pagesLab. Activity Mycologyuci marleyPas encore d'évaluation
- Lesson 13: The Functions and Activities of The Laboratory Sample Reception AreaDocument25 pagesLesson 13: The Functions and Activities of The Laboratory Sample Reception AreaAngel joyce ValenciaPas encore d'évaluation
- Microbiology Lecture 1 - Structure, Classification and MorphologyDocument4 pagesMicrobiology Lecture 1 - Structure, Classification and MorphologyAldwin BagtasPas encore d'évaluation
- Prelims Week 3 - Urinalysis - TransDocument16 pagesPrelims Week 3 - Urinalysis - TransLoro JDPas encore d'évaluation
- 1 VenipunctureDocument42 pages1 VenipunctureQuennie Abellon QuimanPas encore d'évaluation
- Histopath Lec (Module 1) : Iintroduction To PathologyDocument17 pagesHistopath Lec (Module 1) : Iintroduction To PathologyAngela ReyesPas encore d'évaluation
- Body FluidsDocument81 pagesBody FluidsAris ResurreccionPas encore d'évaluation
- Compiled Quizes AubfDocument39 pagesCompiled Quizes AubfCharmaine BoloPas encore d'évaluation
- PMLS 2 PrelimsDocument55 pagesPMLS 2 PrelimsCassey Stephane PinedaPas encore d'évaluation
- Bacteriology Lab 2 - Instruments Used in Bacteriology LaboratoryDocument1 pageBacteriology Lab 2 - Instruments Used in Bacteriology LaboratoryJiro Anderson EscañaPas encore d'évaluation
- Clinical Chemistry 2 ENZYMES. MEDICAL TECHNOLOGYDocument4 pagesClinical Chemistry 2 ENZYMES. MEDICAL TECHNOLOGYBib imbapPas encore d'évaluation
- MTLBE Internship Assessment QuizDocument2 pagesMTLBE Internship Assessment QuizAngela LaglivaPas encore d'évaluation
- MLT503 - L2 - General Properties of VirusesDocument51 pagesMLT503 - L2 - General Properties of VirusesMuhammad FirdausPas encore d'évaluation
- Bacteriology PRELIMS PDFDocument225 pagesBacteriology PRELIMS PDFRichell VillacarlosPas encore d'évaluation
- CestodesDocument86 pagesCestodesPidchayathanakorn Paemika0% (1)
- Foundations in Microbiology: Nonspecific Host Defenses TalaroDocument35 pagesFoundations in Microbiology: Nonspecific Host Defenses TalaroOdurPas encore d'évaluation
- L E CellDocument59 pagesL E CellAvi VermaPas encore d'évaluation
- Foundations in Microbiology: The Cocci of Medical Importance TalaroDocument71 pagesFoundations in Microbiology: The Cocci of Medical Importance TalaroOdurPas encore d'évaluation
- Basic Concepts On Laboratory Biosafety and BiosecurityDocument3 pagesBasic Concepts On Laboratory Biosafety and BiosecurityGwynneth EuriccaPas encore d'évaluation
- Venipuncture Complications and Preexamination Variables: RequistionsDocument19 pagesVenipuncture Complications and Preexamination Variables: RequistionsAngel Cascayan Delos SantosPas encore d'évaluation
- 3.2 Acid Fast StainingDocument26 pages3.2 Acid Fast StainingMiguel CuevasPas encore d'évaluation
- Diagnostic Biochemistry. (Ms 1st &2nd Sem.3rd Year) Part-3newDocument94 pagesDiagnostic Biochemistry. (Ms 1st &2nd Sem.3rd Year) Part-3newmatrix_oriPas encore d'évaluation
- Clinical Microscopy 2 Post ExamDocument4 pagesClinical Microscopy 2 Post ExamJaymih Santos AbasoloPas encore d'évaluation
- Group 3 - ParasitologyDocument8 pagesGroup 3 - Parasitologyjulo_05Pas encore d'évaluation
- Diagnostic Procedures For Primary HemostasisDocument2 pagesDiagnostic Procedures For Primary HemostasisAezel CruzPas encore d'évaluation
- F01 Thorax I (Chest and Lungs)Document113 pagesF01 Thorax I (Chest and Lungs)nonelPas encore d'évaluation
- Stool AnalysisDocument8 pagesStool AnalysisAbed AbusalemPas encore d'évaluation
- Safety Security Biosafety Laboratory Biosecurity PerspectiveDocument5 pagesSafety Security Biosafety Laboratory Biosecurity PerspectiveZabdiel Ann SavellanoPas encore d'évaluation
- Gastric FluidDocument4 pagesGastric Fluidchippai22Pas encore d'évaluation
- Unit 11 Arterial PunctureDocument34 pagesUnit 11 Arterial PunctureZoe Rodriguez100% (1)
- Bacterial GrowthDocument83 pagesBacterial Growthashok lakhlanPas encore d'évaluation
- Cytogenetics: Preliminaries: Mccarty Shows That Dna Can Transform BacteriaDocument5 pagesCytogenetics: Preliminaries: Mccarty Shows That Dna Can Transform BacteriaRomie SolacitoPas encore d'évaluation
- Introduction To Medical Microbiology: Mulualem Tadesse (PHD, Assistant Mulualem Tadesse (PHD, AssistantDocument21 pagesIntroduction To Medical Microbiology: Mulualem Tadesse (PHD, Assistant Mulualem Tadesse (PHD, AssistantGemechu TesfaPas encore d'évaluation
- Stanbio Glucose Oxidase Method and Glucose Determination by ProfameDocument2 pagesStanbio Glucose Oxidase Method and Glucose Determination by ProfameQUIAL BINPas encore d'évaluation
- StainsDocument4 pagesStainsMonique ManiwanPas encore d'évaluation
- Inorganic and Organic Chemistry Prelims ReviewerDocument33 pagesInorganic and Organic Chemistry Prelims ReviewerMary Ann C RecañaPas encore d'évaluation
- ISLab P5 - Bacterial Agglutination TestDocument8 pagesISLab P5 - Bacterial Agglutination TestDanielle Anne LambanPas encore d'évaluation
- Defining The Practice of Medical Technology or Clinical Laboratory Science ProfessionDocument27 pagesDefining The Practice of Medical Technology or Clinical Laboratory Science ProfessionKianna TicsayPas encore d'évaluation
- The Intestinal NematodesDocument9 pagesThe Intestinal NematodesdhaineyPas encore d'évaluation
- Syllabus STS New NormalDocument11 pagesSyllabus STS New Normalemmanuel maboloPas encore d'évaluation
- Protozoa: Guanling Wu, Prof. in Dept. Pathogen Biology, Nanjing Medical University, Najing, Jiangsu, ChinaDocument73 pagesProtozoa: Guanling Wu, Prof. in Dept. Pathogen Biology, Nanjing Medical University, Najing, Jiangsu, ChinaUmer RasheedPas encore d'évaluation
- Medical Virology: Introduction To BasicsDocument88 pagesMedical Virology: Introduction To BasicsSutapa PawarPas encore d'évaluation
- HTMLE SEMINAR NOTES DOC. ORTEGA - CompressedDocument35 pagesHTMLE SEMINAR NOTES DOC. ORTEGA - CompressedNISSI JUNE T. UNGABPas encore d'évaluation
- Quality Assurance in BacteriologyDocument28 pagesQuality Assurance in BacteriologyAuguz Francis Acena50% (2)
- Course Assessment 1.0 Forensic EssayDocument11 pagesCourse Assessment 1.0 Forensic EssayNevado Jericho Echo100% (1)
- Pneumonia II MicrobesDocument15 pagesPneumonia II MicrobespuniariPas encore d'évaluation
- Lower Airway DiseasesDocument70 pagesLower Airway DiseasesAavash PradhanPas encore d'évaluation
- InfluDocument32 pagesInflusaurabhdhakedgPas encore d'évaluation
- Fisika BioelektrikDocument50 pagesFisika BioelektrikFachriza EffendiPas encore d'évaluation
- Aromatherapy: Does It Work ?Document15 pagesAromatherapy: Does It Work ?Fachriza EffendiPas encore d'évaluation
- Kuliah AnatomiDocument45 pagesKuliah AnatomiFachriza EffendiPas encore d'évaluation
- Medical SpeakingDocument3 pagesMedical SpeakingFachriza EffendiPas encore d'évaluation
- Personal HigientDocument5 pagesPersonal HigientFachriza EffendiPas encore d'évaluation
- Pelatihan TB MDRDocument178 pagesPelatihan TB MDRFachriza EffendiPas encore d'évaluation
- Kuliah AnatomiDocument20 pagesKuliah AnatomiFachriza EffendiPas encore d'évaluation
- Soal Pretest AnatomiDocument22 pagesSoal Pretest AnatomiFachriza EffendiPas encore d'évaluation
- Skeletal SystemDocument42 pagesSkeletal SystemFachriza EffendiPas encore d'évaluation
- Skeletal SystemDocument4 pagesSkeletal SystemFachriza EffendiPas encore d'évaluation
- Axial SkeletonDocument34 pagesAxial SkeletonFachriza EffendiPas encore d'évaluation
- Appendicular SkeletonDocument23 pagesAppendicular SkeletonFachriza Effendi100% (1)
- Bagan MikroDocument14 pagesBagan MikroFachriza EffendiPas encore d'évaluation
- Komunikasi Sel SelaDocument46 pagesKomunikasi Sel SelaFachriza EffendiPas encore d'évaluation
- Sesi 1Document22 pagesSesi 1Fachriza EffendiPas encore d'évaluation
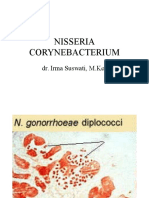
- Nisseria Corynebacterium: Dr. Irma Suswati, M.KesDocument10 pagesNisseria Corynebacterium: Dr. Irma Suswati, M.KesFachriza EffendiPas encore d'évaluation
- Epidemiologi AnalitikDocument36 pagesEpidemiologi AnalitikFachriza EffendiPas encore d'évaluation
- Public Health SurveillanceDocument18 pagesPublic Health SurveillanceFachriza EffendiPas encore d'évaluation
- Investigating An Outbreak (Epidemic)Document36 pagesInvestigating An Outbreak (Epidemic)Fachriza Effendi100% (1)
- Epidemiologi AnalitikDocument36 pagesEpidemiologi AnalitikFachriza EffendiPas encore d'évaluation
- SKRENING UntukDocument30 pagesSKRENING Untukdarkim777Pas encore d'évaluation
- Research Design (Rancang Penelitian) : Siswanto, MD, MSCDocument55 pagesResearch Design (Rancang Penelitian) : Siswanto, MD, MSCFachriza EffendiPas encore d'évaluation
- Research Design (Rancang Penelitian)Document48 pagesResearch Design (Rancang Penelitian)Fachriza EffendiPas encore d'évaluation
- BiostatistikDocument8 pagesBiostatistikFachriza EffendiPas encore d'évaluation
- Research Design (Rancang Penelitian) : Siswanto, MD, MSCDocument55 pagesResearch Design (Rancang Penelitian) : Siswanto, MD, MSCFachriza EffendiPas encore d'évaluation
- DR - Shinta Neuropati DiabetikDocument32 pagesDR - Shinta Neuropati DiabetikHamdan Muarifin PutraPas encore d'évaluation
- EPIDemiologi BPK SiswantoDocument47 pagesEPIDemiologi BPK SiswantoFachriza EffendiPas encore d'évaluation
- Communicable DiseasesDocument176 pagesCommunicable DiseasesKimsha ConcepcionPas encore d'évaluation
- IF4.02 Molecular Pathogenesis of Klebsiella Pneumoniae PDFDocument36 pagesIF4.02 Molecular Pathogenesis of Klebsiella Pneumoniae PDFdindaPas encore d'évaluation
- MALARIADocument8 pagesMALARIAMohmmadRjab SederPas encore d'évaluation
- Patho DHFDocument2 pagesPatho DHFPhillip GoPas encore d'évaluation
- Ospe ParasitologyDocument19 pagesOspe Parasitologyaimi Batrisyia100% (1)
- Culture MediaDocument4 pagesCulture MediaHabibur RahamanPas encore d'évaluation
- Apicomplexa (Sporozoa) 5.1general Future and ClassificationDocument10 pagesApicomplexa (Sporozoa) 5.1general Future and Classificationtedela gulumaPas encore d'évaluation
- Microchem Non GLP ASTM E1052 Study Report NG14797Document6 pagesMicrochem Non GLP ASTM E1052 Study Report NG14797MaryDianne RamosPas encore d'évaluation
- Scabies MoreDocument5 pagesScabies MoreArva Glazel Defensor GallofinPas encore d'évaluation
- DHQ Flowcharts v2.0Document49 pagesDHQ Flowcharts v2.0SabirAli SayyedPas encore d'évaluation
- Training Slides HSE-OH-ST10 Biological HazardsDocument18 pagesTraining Slides HSE-OH-ST10 Biological HazardsAbdul Malik AnsariPas encore d'évaluation
- Chicken PoxDocument26 pagesChicken Poxlfams100% (1)
- E2871-13 Standard Test Method For Evaluating DisinfectDocument6 pagesE2871-13 Standard Test Method For Evaluating DisinfectA MusaverPas encore d'évaluation
- A Brief History of Vaccines and Vaccination.Document20 pagesA Brief History of Vaccines and Vaccination.sameer100% (2)
- AIDS/HIV An Overview 1Document7 pagesAIDS/HIV An Overview 1tiffrenfitPas encore d'évaluation
- Activity Design Mrsia 2018Document3 pagesActivity Design Mrsia 2018RJay Mon MarcosPas encore d'évaluation
- Lloyd Rice - Distribution - of - Heartwater - in - Cattle - in - Gokwe North District ZimbabweDocument32 pagesLloyd Rice - Distribution - of - Heartwater - in - Cattle - in - Gokwe North District ZimbabweLloyd RicePas encore d'évaluation
- Aerobic Gram Positive BacilliDocument36 pagesAerobic Gram Positive BacilliMac Kevin MandapPas encore d'évaluation
- Pneumonia Si Pleurezia Parapneumonica: Agentii Etiologici Cei Mai FrecventiDocument2 pagesPneumonia Si Pleurezia Parapneumonica: Agentii Etiologici Cei Mai FrecventiCatalina Andreea CucutaPas encore d'évaluation
- Man Bahadur Rana BPH, Acas, NepalDocument34 pagesMan Bahadur Rana BPH, Acas, NepalDipankar NathPas encore d'évaluation
- AnaplasmaDocument22 pagesAnaplasmaSomesh SharmaPas encore d'évaluation
- Virus Replication StrategyDocument6 pagesVirus Replication StrategyShreyash Raj100% (1)
- Advanced Techniques in Diagnostic MicrobiologyDocument14 pagesAdvanced Techniques in Diagnostic MicrobiologyTumabang DivinePas encore d'évaluation
- Detailed Drug StudyDocument5 pagesDetailed Drug StudyKarl Vincent SosoPas encore d'évaluation
- Introduction CASE STUDYDocument3 pagesIntroduction CASE STUDYDavid CalaloPas encore d'évaluation
- CDC: Improving Communications Around Vaccine Breakthrough and Vaccine EffectivenessDocument25 pagesCDC: Improving Communications Around Vaccine Breakthrough and Vaccine EffectivenessCNBC.com100% (1)
- VILSAN CatalougeDocument97 pagesVILSAN CatalougeSầu VePas encore d'évaluation
- Acute Bacterial MeningitisDocument15 pagesAcute Bacterial MeningitisOana StefanPas encore d'évaluation
- Infectious Diseases CM 231Document45 pagesInfectious Diseases CM 231Simina ÎntunericPas encore d'évaluation
- Colibacillosis in LayersDocument10 pagesColibacillosis in LayersKarki KedarPas encore d'évaluation