Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Skeletal System 1Document30 pagesSkeletal System 1api-298936084100% (1)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- CRANIOFACIAL Anomalies in ChildrenDocument55 pagesCRANIOFACIAL Anomalies in ChildrenDr. Shirley Mausi N.Pas encore d'évaluation
- Stages of Prenatal DevelopmentDocument4 pagesStages of Prenatal DevelopmentPDGJHD100% (1)
- Lab 5 Coombs TestsDocument26 pagesLab 5 Coombs TestsJennifer DixonPas encore d'évaluation
- Oncology Nursing NotesDocument12 pagesOncology Nursing Notesjoyrena ochondra100% (6)
- (Book 1) : Career Paths: Physiotherapy - GlossaryDocument15 pages(Book 1) : Career Paths: Physiotherapy - Glossarygab77Pas encore d'évaluation
- Basics in Medical EducationDocument5 pagesBasics in Medical EducationLia0% (1)
- Rcog PDFDocument17 pagesRcog PDFLiaPas encore d'évaluation
- Kelumpuhan Nervus Fasialis PeriferDocument28 pagesKelumpuhan Nervus Fasialis PeriferFahryza Akbar Diyanto FirmansyahPas encore d'évaluation
- 997 3118 1 PBDocument11 pages997 3118 1 PBSasono HanditoPas encore d'évaluation
- Ipi 10527Document8 pagesIpi 10527LiaPas encore d'évaluation
- Supplemental Digital Content 1: Pubmed Search StrategyDocument10 pagesSupplemental Digital Content 1: Pubmed Search StrategyLiaPas encore d'évaluation
- kjr-US For Benign and Maligna PDFDocument9 pageskjr-US For Benign and Maligna PDFLiaPas encore d'évaluation
- kjr-US For Benign and Maligna PDFDocument9 pageskjr-US For Benign and Maligna PDFLiaPas encore d'évaluation
- Varicella Guidance PDFDocument58 pagesVaricella Guidance PDFLiza Aulia PutriPas encore d'évaluation
- Health Services Are GuaranteedDocument1 pageHealth Services Are GuaranteedLiaPas encore d'évaluation
- Varicella VaksinDocument2 pagesVaricella VaksinPutri AmengkutyasPas encore d'évaluation
- Introduction Block 2 2011 10Document20 pagesIntroduction Block 2 2011 10LiaPas encore d'évaluation
- This Movie Is The Romantic DramaDocument1 pageThis Movie Is The Romantic DramaLiaPas encore d'évaluation
- Taking Medicine Before MealsDocument6 pagesTaking Medicine Before MealsLiaPas encore d'évaluation
- Skenario PLENARY CASE Blok 3 KuDocument3 pagesSkenario PLENARY CASE Blok 3 KuLiaPas encore d'évaluation
- 169 314 1 SMDocument9 pages169 314 1 SMDian SuasanaPas encore d'évaluation
- Brain Attack Definition An Did of Stroke Present A It OnDocument36 pagesBrain Attack Definition An Did of Stroke Present A It OnchirahmawatiPas encore d'évaluation
- Urodynamics Griffiths ICS 2014Document198 pagesUrodynamics Griffiths ICS 2014nadalPas encore d'évaluation
- Moving Through The Digestive System Writing AssignmentDocument4 pagesMoving Through The Digestive System Writing AssignmentJoy JonesPas encore d'évaluation
- Sample Detailed Lesson PlanDocument11 pagesSample Detailed Lesson PlanImee-leen Eusebio-MateoPas encore d'évaluation
- Quarter 2 - Module 3Document53 pagesQuarter 2 - Module 3Jay AlbaytarPas encore d'évaluation
- Complementar - The Prevalence of Alcoholic Cerebellar AtrophyDocument9 pagesComplementar - The Prevalence of Alcoholic Cerebellar AtrophySantiago AlzatePas encore d'évaluation
- International 3Document3 pagesInternational 3daffunkmadansyahPas encore d'évaluation
- Essentials of Anatomy and Physiology 6th Edition Martini Solutions ManualDocument12 pagesEssentials of Anatomy and Physiology 6th Edition Martini Solutions Manualscarletba4cc100% (34)
- Feoutal AddDocument9 pagesFeoutal AddDHUPGURI DIAGNOSTICPas encore d'évaluation
- MCQ Blood Physiology SermadDocument22 pagesMCQ Blood Physiology SermadAsif Hanif50% (4)
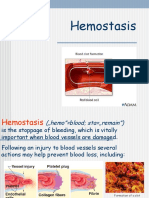
- Lecture HemostasisDocument28 pagesLecture HemostasisЛариса ТкачеваPas encore d'évaluation
- Heart and Circulation Test: NameDocument12 pagesHeart and Circulation Test: NamezipperPas encore d'évaluation
- Kode TopografiDocument69 pagesKode TopografiMUHAMMAD RASYID RPas encore d'évaluation
- 4 Notes Anatomy and Physiology MariebDocument12 pages4 Notes Anatomy and Physiology Mariebmine2515Pas encore d'évaluation
- Bone Marrow: Andy Mclarnon, University of Birmingham, UkDocument2 pagesBone Marrow: Andy Mclarnon, University of Birmingham, Uknavita guptaPas encore d'évaluation
- GR-5 ScienceDocument354 pagesGR-5 SciencePrecious RubaPas encore d'évaluation
- 10 Diseases - and - Immunity - Igcse Cie Biology - Ext Theory QP - UpdatedDocument9 pages10 Diseases - and - Immunity - Igcse Cie Biology - Ext Theory QP - Updatedmaryam2024igcsePas encore d'évaluation
- Cell Summative ReviewDocument5 pagesCell Summative Reviewapi-422959755100% (1)
- Maternal ReviewerDocument9 pagesMaternal ReviewerMary Reigns BuhatPas encore d'évaluation
- Exchange Surfaces 2 QPDocument13 pagesExchange Surfaces 2 QPSaaleh AbanurPas encore d'évaluation
- Body (مفردات جسم الإنسان)Document6 pagesBody (مفردات جسم الإنسان)Armylova OfficialPas encore d'évaluation
- CASE REPORT Dr. Arie Polim, SpOG FinalDocument50 pagesCASE REPORT Dr. Arie Polim, SpOG FinalpriskavkPas encore d'évaluation
- 1 - The Skin's Function PDFDocument9 pages1 - The Skin's Function PDFskoahPas encore d'évaluation
- Blood and Circulation PDFDocument47 pagesBlood and Circulation PDFeric sivaneshPas encore d'évaluation
- AssignmentLec2 DimnatangDocument2 pagesAssignmentLec2 DimnatangFatimah DimnatangPas encore d'évaluation