Vous aimerez peut-être aussi
- Dept. of Medical and Clinical Biochemistry Upjš in Košice, Medical Faculty Eva Ďurovcová, Md. Phd. 5 GM CLBDocument48 pagesDept. of Medical and Clinical Biochemistry Upjš in Košice, Medical Faculty Eva Ďurovcová, Md. Phd. 5 GM CLBPaulina PaskeviciutePas encore d'évaluation
- Relationship of Nutrition To Blood Glucose Control: Arline Mcdonald, Ph.D. December 4, 2001Document39 pagesRelationship of Nutrition To Blood Glucose Control: Arline Mcdonald, Ph.D. December 4, 2001Zy HoePas encore d'évaluation
- 14 - Blood Glucose HomeostasisDocument34 pages14 - Blood Glucose HomeostasischeckmatePas encore d'évaluation
- Lab Tests For DM WRNDocument45 pagesLab Tests For DM WRNLiaApprilia Kartinii Cupcupcuap ElvenadoPas encore d'évaluation
- Lecture 2 - Blood SugarDocument11 pagesLecture 2 - Blood SugartagmanPas encore d'évaluation
- Glucagon and Its Metabolic EffectsDocument31 pagesGlucagon and Its Metabolic EffectsnikenPas encore d'évaluation
- DPP 4Document20 pagesDPP 4Genix PharmaPas encore d'évaluation
- Week 26 James Banting Insulin: TissueDocument12 pagesWeek 26 James Banting Insulin: Tissuedragtoss2Pas encore d'évaluation
- Farmakologi Diabetes Melitus: Deni SetiawanDocument66 pagesFarmakologi Diabetes Melitus: Deni SetiawanNoor Hikmah FajarPas encore d'évaluation
- 23.Keto-Asidosis DiabetikDocument30 pages23.Keto-Asidosis DiabetikmutiaPas encore d'évaluation
- GI TrackDocument125 pagesGI TrackAndika HPas encore d'évaluation
- Hormones in Metabolism (DR - Ani Retno)Document45 pagesHormones in Metabolism (DR - Ani Retno)AciPas encore d'évaluation
- Random Blood Sugar Measurement: Lab Class 4Document11 pagesRandom Blood Sugar Measurement: Lab Class 4sontori miliPas encore d'évaluation
- Type I Diabetes MellitesDocument71 pagesType I Diabetes MellitesMuthu LakshmiPas encore d'évaluation
- Nutrisi Pada DMDocument48 pagesNutrisi Pada DMalwiPas encore d'évaluation
- Diabetes Mellitus: Presentation By: Dr. Petrescu Elena Dr. Stanescu RalucaDocument41 pagesDiabetes Mellitus: Presentation By: Dr. Petrescu Elena Dr. Stanescu RalucaMarcoPas encore d'évaluation
- DR Moat Paediatric BochemistryDocument62 pagesDR Moat Paediatric Bochemistrymonday125Pas encore d'évaluation
- Diabetic Foot UlcerDocument93 pagesDiabetic Foot UlcerMichael AdjeiPas encore d'évaluation
- Lecture 2 Clinical BiochemistryDocument41 pagesLecture 2 Clinical BiochemistryTilihoi Doru Jr.Pas encore d'évaluation
- Carbohydrate 1Document60 pagesCarbohydrate 1jahahn.t.sullivanPas encore d'évaluation
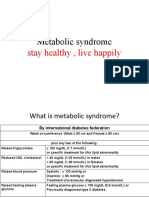
- Metabolic Syndrome: Stay Healthy, Live HappilyDocument32 pagesMetabolic Syndrome: Stay Healthy, Live HappilykomalscientistPas encore d'évaluation
- Diabetes Mellitus SeminarDocument35 pagesDiabetes Mellitus SeminarAnkush SinglaPas encore d'évaluation
- Pharmacotherapy of Diabetes MellitusDocument120 pagesPharmacotherapy of Diabetes MellitusElfiaNeswitaPas encore d'évaluation
- Biochemical Changes of Diabetes MellitusDocument4 pagesBiochemical Changes of Diabetes MellitusGerardLum100% (3)
- Drug Therapy in Diabetes: Dr. Joe George MD, DNB, DM (Endocrinology) Department of Endocrinology, KEM Hospital, MumbaiDocument44 pagesDrug Therapy in Diabetes: Dr. Joe George MD, DNB, DM (Endocrinology) Department of Endocrinology, KEM Hospital, Mumbaijoe georgePas encore d'évaluation
- Diabetes MellitusDocument77 pagesDiabetes MellitusAshok100% (5)
- 4 Diabetes MellitusDocument26 pages4 Diabetes MellitusnomiskemalPas encore d'évaluation
- The Role of Rapid Acting Analogue in Basal-Bolus StrategyDocument25 pagesThe Role of Rapid Acting Analogue in Basal-Bolus StrategyYennySuryaniPas encore d'évaluation
- 췌장호르몬과 당뇨Document28 pages췌장호르몬과 당뇨missoni0408Pas encore d'évaluation
- 2023 Diabetes Mellitus L1 To L8 SVDocument267 pages2023 Diabetes Mellitus L1 To L8 SVThubelihle ZuluPas encore d'évaluation
- Metabolic Syndrome: SMF Ilmu Penyakit Dalam RSD Gunung Jati Kota CirebonDocument50 pagesMetabolic Syndrome: SMF Ilmu Penyakit Dalam RSD Gunung Jati Kota CirebonFina Sudarni SPas encore d'évaluation
- Anatomy of Pancreas and Glucose Homeostasis: DR - Sasikala. JDocument48 pagesAnatomy of Pancreas and Glucose Homeostasis: DR - Sasikala. JsaranpcPas encore d'évaluation
- DiabetesDocument2 pagesDiabetesAna Delia LabianoPas encore d'évaluation
- Physio Correl - Insulin and GlucagonDocument33 pagesPhysio Correl - Insulin and GlucagonDan Tristam MicabaloPas encore d'évaluation
- PancreasDocument100 pagesPancreasb0t.mc.sundayPas encore d'évaluation
- Hyperglycemic Crises: ReferralDocument51 pagesHyperglycemic Crises: ReferralKokohPas encore d'évaluation
- For Nursing1604-212: Department of Physiology College of Medicine Imam Abdulrahman Bin Faisal UniversityDocument18 pagesFor Nursing1604-212: Department of Physiology College of Medicine Imam Abdulrahman Bin Faisal UniversityARAK AldarwishPas encore d'évaluation
- End PancreasDocument29 pagesEnd Pancreasahmed alkramyPas encore d'évaluation
- Diabetes MellitusDocument91 pagesDiabetes MellitusInnocentPas encore d'évaluation
- Diabetes - Oral KnowledgeDocument19 pagesDiabetes - Oral KnowledgeKSeegurPas encore d'évaluation
- Diabetes Dan Penyakit Endokrin DR Sebastian JobulDocument40 pagesDiabetes Dan Penyakit Endokrin DR Sebastian JobulMiranda RozziqaPas encore d'évaluation
- Endocrine Part1Document6 pagesEndocrine Part1ahmed nasserPas encore d'évaluation
- Obesitas Mets DMDocument47 pagesObesitas Mets DMFathimah UswahPas encore d'évaluation
- Biochemistry Lecture 8 Final PPT - B&WDocument35 pagesBiochemistry Lecture 8 Final PPT - B&Wsamyu827Pas encore d'évaluation
- Carbohydrate DisorderDocument74 pagesCarbohydrate DisorderEric YewPas encore d'évaluation
- Obat Antidiabetes: Hernita TaurustyaDocument70 pagesObat Antidiabetes: Hernita TaurustyaHernita TaurustyaPas encore d'évaluation
- Pathophysiology Notes: Diabetes Mellitus Is A Group of Metabolic Disorders Characterized HyperglycemiaDocument14 pagesPathophysiology Notes: Diabetes Mellitus Is A Group of Metabolic Disorders Characterized HyperglycemiaHaifa ibrahimPas encore d'évaluation
- Liver (Hati) ZLDocument27 pagesLiver (Hati) ZLpafaniPas encore d'évaluation
- Pros and ConsDocument21 pagesPros and ConsBarlian AlamudiPas encore d'évaluation
- Coma Hyperglycemic Hyperosmolar NonketoticDocument10 pagesComa Hyperglycemic Hyperosmolar NonketoticD An0% (1)
- Farmakoterapi I Diabetes Melitus (DM)Document17 pagesFarmakoterapi I Diabetes Melitus (DM)Ekhi RezkiPas encore d'évaluation
- OBAT ANTI-DIABETES - Hernita - 2019Document70 pagesOBAT ANTI-DIABETES - Hernita - 2019Hernita TaurustyaPas encore d'évaluation
- Acute Complications of DM ESS 2016Document41 pagesAcute Complications of DM ESS 2016teodordragnev1Pas encore d'évaluation
- Mild Diabetic Ketoacidosis2Document10 pagesMild Diabetic Ketoacidosis2GorgiePas encore d'évaluation
- Diabetes Mellitus: Nhamier M. Jikiri, RN, MD, FPCP Internal MedicineDocument27 pagesDiabetes Mellitus: Nhamier M. Jikiri, RN, MD, FPCP Internal MedicineNursidar Pascual MukattilPas encore d'évaluation
- DM Hiperglikemia 20-9-18Document27 pagesDM Hiperglikemia 20-9-18JessicaPas encore d'évaluation
- Diabetes Mellitus: Regulation of Blood GlucoseDocument65 pagesDiabetes Mellitus: Regulation of Blood GlucoseReggae BautistaPas encore d'évaluation
- Physiology DiabetesDocument48 pagesPhysiology Diabetesrajesh g100% (1)
- 2020 The Essential Diets - All Diets in One Book - Ketogenic, Mediterranean, Mayo, Zone Diet, High Protein, Vegetarian, Vegan, Detox, Paleo, Alkaline Diet and Much More: COOKBOOK, #2D'Everand2020 The Essential Diets - All Diets in One Book - Ketogenic, Mediterranean, Mayo, Zone Diet, High Protein, Vegetarian, Vegan, Detox, Paleo, Alkaline Diet and Much More: COOKBOOK, #2Pas encore d'évaluation
- Diabetic Recipes for One and TwoD'EverandDiabetic Recipes for One and TwoÉvaluation : 3 sur 5 étoiles3/5 (1)
- Presentation TitleDocument4 pagesPresentation TitleArlin Chyntia DewiPas encore d'évaluation
- Stagii - Nefrologie Stagiu UnuDocument7 pagesStagii - Nefrologie Stagiu UnuIoana DiaconuPas encore d'évaluation
- Neuro - Miscari InvoluntareDocument2 pagesNeuro - Miscari InvoluntareIoana DiaconuPas encore d'évaluation
- Aaa 43211000 FCGVHDocument1 pageAaa 43211000 FCGVHIoana DiaconuPas encore d'évaluation
- FC GVHDocument1 pageFC GVHIoana DiaconuPas encore d'évaluation
- Presentation 1Document3 pagesPresentation 1Ioana DiaconuPas encore d'évaluation
- HDInferioara PpsDocument25 pagesHDInferioara PpsIoana DiaconuPas encore d'évaluation
- Proteomics in Nephrology. Towards Clinical Applications (2008) PDFDocument213 pagesProteomics in Nephrology. Towards Clinical Applications (2008) PDFIoana DiaconuPas encore d'évaluation
- Preclinical Evaluation of The Stability, Safety, and Efficacy of CD101, A Novel EchinocandinDocument8 pagesPreclinical Evaluation of The Stability, Safety, and Efficacy of CD101, A Novel EchinocandinAayush SinghPas encore d'évaluation
- Kiran Kumar Sahu - ELDocument5 pagesKiran Kumar Sahu - ELStupid IdiotPas encore d'évaluation
- Obstetric Case Study CesarianDocument16 pagesObstetric Case Study CesarianRazan NasereddinePas encore d'évaluation
- Link Download Ebook Anatomy and PhysiologyDocument87 pagesLink Download Ebook Anatomy and Physiologyarif100% (1)
- Drugs Used For GlaucomaDocument40 pagesDrugs Used For GlaucomaAgust SalimPas encore d'évaluation
- Association Between Breastfeeding Patterns and Type 1 Diabetes Among ChildrenDocument6 pagesAssociation Between Breastfeeding Patterns and Type 1 Diabetes Among ChildrenHarun joel tatipataPas encore d'évaluation
- 260 QuestionsDocument42 pages260 QuestionsMaryjoy Mertalla50% (4)
- Medical For Athletes 2Document2 pagesMedical For Athletes 2Lian Christine GagantePas encore d'évaluation
- Vakcinacija U Nemackoj Germany Ip VakcinaDocument3 pagesVakcinacija U Nemackoj Germany Ip VakcinaNikola IvankovicPas encore d'évaluation
- Clinical Manual For PubliC HealtH Dentistry and PraCtiCal reCorD Book PDFDocument322 pagesClinical Manual For PubliC HealtH Dentistry and PraCtiCal reCorD Book PDFSweet SumanPas encore d'évaluation
- Four Handed Dentistry: An Indispensable Part For Efficient Clinical PracticeDocument6 pagesFour Handed Dentistry: An Indispensable Part For Efficient Clinical PracticeDevi NingrumPas encore d'évaluation
- Orphan DrugsDocument16 pagesOrphan Drugssakumar5678Pas encore d'évaluation
- Department of Education: Health Declaration FormDocument2 pagesDepartment of Education: Health Declaration FormCherrie Lynne AlbisPas encore d'évaluation
- Mental Retardation Lesson PlanDocument10 pagesMental Retardation Lesson Plansp2056251Pas encore d'évaluation
- Male Hypogonadism: Approval Number: G.MKT - GM.MH.04.2018.0513Document19 pagesMale Hypogonadism: Approval Number: G.MKT - GM.MH.04.2018.0513Billi Siddiqui100% (1)
- Non-Medical Endoscopists: British Society of GastroenterologyDocument11 pagesNon-Medical Endoscopists: British Society of GastroenterologyScott MackenziePas encore d'évaluation
- Np2 Recalls 4Document7 pagesNp2 Recalls 4AhrisJeannine EscuadroPas encore d'évaluation
- Forbidden Cures E Book DR SircusDocument381 pagesForbidden Cures E Book DR Sircusvitaolga7100% (18)
- Sales Brochure Cancer Cover 05-03-2020 CC PDFDocument7 pagesSales Brochure Cancer Cover 05-03-2020 CC PDFHeera KardongPas encore d'évaluation
- Munchies BrochureDocument28 pagesMunchies BrochureIbrahim Diaz LazoPas encore d'évaluation
- ĐA ĐỀ 124 (VIP 23)Document23 pagesĐA ĐỀ 124 (VIP 23)thanhnam2982005Pas encore d'évaluation
- DAFTAR PUSTAKA Kanker EndometriumDocument3 pagesDAFTAR PUSTAKA Kanker EndometriumRiri AmalinaPas encore d'évaluation
- Biosafety Levels: Submitted To Submitted byDocument16 pagesBiosafety Levels: Submitted To Submitted bySheikh FirdousPas encore d'évaluation
- Daftar Pustaka - 4Document3 pagesDaftar Pustaka - 4PascaIKM STIKes KuninganPas encore d'évaluation
- Pylorus Preservation Pancreatectomy or Not: Ulla Klaiber, Pascal Probst, Markus W. Büchler, Thilo HackertDocument8 pagesPylorus Preservation Pancreatectomy or Not: Ulla Klaiber, Pascal Probst, Markus W. Büchler, Thilo HackertHiroj BagdePas encore d'évaluation
- Jurnal Skripsi Sabam GultomDocument3 pagesJurnal Skripsi Sabam GultomDavid Galatia TambaPas encore d'évaluation
- RCP 2020Document51 pagesRCP 2020Jose Jhampool Quevedo LealPas encore d'évaluation
- College of Health Sciences: Urdaneta City UniversityDocument2 pagesCollege of Health Sciences: Urdaneta City UniversityDan Dan ManaoisPas encore d'évaluation
- Case Reports in Women's Health: Tanja Baltus Maria Luisa MartinDocument2 pagesCase Reports in Women's Health: Tanja Baltus Maria Luisa MartinDavid LacostePas encore d'évaluation
- IAU Logbook Core 6weeksDocument7 pagesIAU Logbook Core 6weeksbajariaaPas encore d'évaluation