Vous aimerez peut-être aussi
- Gaulish DictionaryDocument4 pagesGaulish DictionarywoodwysePas encore d'évaluation
- Pharma CardsDocument5 pagesPharma CardsazanchePas encore d'évaluation
- Problem With The PassageDocument3 pagesProblem With The PassageLuiciaPas encore d'évaluation
- Pulmonology Step2 CKDocument22 pagesPulmonology Step2 CKsarwat86% (7)
- Anand's Human Anatomy For Dental Students, 3rd EditionDocument762 pagesAnand's Human Anatomy For Dental Students, 3rd Editionviaerea100% (4)
- Allergic Rhinitis and RhinosinusitisDocument53 pagesAllergic Rhinitis and RhinosinusitisSinta FiraniPas encore d'évaluation
- Oxygen Therapy CBPGDocument44 pagesOxygen Therapy CBPGUri Mora100% (2)
- Oxygen Therapy, Trach Care and SuctioningDocument44 pagesOxygen Therapy, Trach Care and SuctioningEmily Boehmer100% (1)
- Abo Case Final Study-LatestDocument56 pagesAbo Case Final Study-LatestJonathan DiazPas encore d'évaluation
- Drug Study - Amiodaron HydrochlorideDocument4 pagesDrug Study - Amiodaron HydrochlorideTwinkle SalongaPas encore d'évaluation
- Acute Treatment of Hypocalcaemia (Adults)Document2 pagesAcute Treatment of Hypocalcaemia (Adults)Ahed WarwarPas encore d'évaluation
- TheophyllineDocument27 pagesTheophyllineAci LusianaPas encore d'évaluation
- Asthma and Other Respiratory Medications DefindDocument4 pagesAsthma and Other Respiratory Medications DefindKiran ManojPas encore d'évaluation
- Case Study On Seizure Disorder On InfantsDocument6 pagesCase Study On Seizure Disorder On InfantsarturogarcesjrPas encore d'évaluation
- Diamond-Blackfan Anemia Is A DisorderDocument22 pagesDiamond-Blackfan Anemia Is A DisorderDarem SoPas encore d'évaluation
- 3 OB 1 - Hypertensive DisordersDocument5 pages3 OB 1 - Hypertensive DisordersIrene FranzPas encore d'évaluation
- Fetal Circulation...Document2 pagesFetal Circulation...Ezra Dizon Manzano100% (1)
- Croup PathwayDocument30 pagesCroup Pathwayshluly23Pas encore d'évaluation
- Phenylephrine: 1568 Cough Suppressants Expectorants Mucolytics and Nasal DecongestantsDocument2 pagesPhenylephrine: 1568 Cough Suppressants Expectorants Mucolytics and Nasal DecongestantsRanny LaidasuriPas encore d'évaluation
- Carbetocin For The Prevention of Postpartum Hemorrhage A Systematic ReviewDocument7 pagesCarbetocin For The Prevention of Postpartum Hemorrhage A Systematic ReviewOscar Gregorio Coronado MacdanielPas encore d'évaluation
- EpinephrineDocument16 pagesEpinephrineBrad Pitt-HongPas encore d'évaluation
- Salbuterol Generic NameDocument4 pagesSalbuterol Generic NamejuniePas encore d'évaluation
- DigoxinDocument6 pagesDigoxinZiedTrikiPas encore d'évaluation
- Drug StudyDocument8 pagesDrug Studysarah1217Pas encore d'évaluation
- Surfactant NeonatologyDocument19 pagesSurfactant NeonatologyMbabazi Theos100% (1)
- Paromomycin SulfateDocument3 pagesParomomycin SulfateRita RodriguesPas encore d'évaluation
- Protein ChemistryDocument11 pagesProtein ChemistryCarmina DinerosPas encore d'évaluation
- Neonatal HypoglyDocument31 pagesNeonatal HypoglyAli FalihPas encore d'évaluation
- Upper GI Tract (Stomach)Document5 pagesUpper GI Tract (Stomach)NAWAB PHOTOCOPYPas encore d'évaluation
- Folic Acid PDFDocument2 pagesFolic Acid PDFmohammadPas encore d'évaluation
- Process RecordingDocument8 pagesProcess RecordingjoannePas encore d'évaluation
- NCM 109-Cerebral PalsyDocument36 pagesNCM 109-Cerebral PalsyLeigh Ann Prosyne LozadaPas encore d'évaluation
- Perioperative HypothermiaDocument4 pagesPerioperative Hypothermiasri utari masyitahPas encore d'évaluation
- Inhaled Nitric OxideDocument27 pagesInhaled Nitric OxideLilian FloresPas encore d'évaluation
- Nonninvasive MonitoringDocument6 pagesNonninvasive MonitoringmardatillahPas encore d'évaluation
- Oxygen TherapyDocument20 pagesOxygen TherapyBeri NyuydzefonPas encore d'évaluation
- OxygenDocument34 pagesOxygenSamson AyalewPas encore d'évaluation
- LTOT Home Oxygen Therapy - StatPearls - NCBI BookshelfDocument5 pagesLTOT Home Oxygen Therapy - StatPearls - NCBI Bookshelfrbatjun576Pas encore d'évaluation
- COPDDocument42 pagesCOPDAnoos rabayarabayaPas encore d'évaluation
- Oxygen TherapyDocument34 pagesOxygen Therapysarahsheikh28100% (5)
- 1 6 - Oxygen-TherapyDocument62 pages1 6 - Oxygen-TherapyJUSTIN ALZATEPas encore d'évaluation
- Care of Clients With Problems in OxygenationDocument8 pagesCare of Clients With Problems in OxygenationRed StohlPas encore d'évaluation
- Physiology of Oxygen TransportDocument37 pagesPhysiology of Oxygen TransportRajitha SiriwardenaPas encore d'évaluation
- 5 Oxygen Therapy& DevicesDocument73 pages5 Oxygen Therapy& Devicesdrnasir31Pas encore d'évaluation
- EMOS Farmacología I Sesion 16Document22 pagesEMOS Farmacología I Sesion 16rafaelPas encore d'évaluation
- Ozone - A New Therapeutic Agent in Vascular Diseases PDFDocument10 pagesOzone - A New Therapeutic Agent in Vascular Diseases PDFullwnPas encore d'évaluation
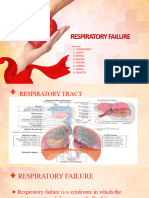
- Respiratory FailureDocument18 pagesRespiratory FailureSai charithaPas encore d'évaluation
- Oxygen Therapy 2012Document34 pagesOxygen Therapy 2012Niko KautsarPas encore d'évaluation
- Medical Gas TherapyDocument84 pagesMedical Gas TherapyJohn Carlo TanPas encore d'évaluation
- Pre-Lab Questions:: Deep Breathing & Coughing Exercises Oxygen TherapyDocument3 pagesPre-Lab Questions:: Deep Breathing & Coughing Exercises Oxygen TherapyaliPas encore d'évaluation
- Oxygen TherapyDocument59 pagesOxygen TherapyRosi AmaliaPas encore d'évaluation
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument11 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDarielStivenRojasCumacoPas encore d'évaluation
- Oxygen Therapy Principles and PracticeDocument34 pagesOxygen Therapy Principles and PracticeMark Anthony AlcantaraPas encore d'évaluation
- Oxygen TherapyDocument44 pagesOxygen TherapyChhabilal BastolaPas encore d'évaluation
- Patterns of RespirationDocument67 pagesPatterns of Respirationsteven hkPas encore d'évaluation
- MonitoringDocument21 pagesMonitoringalfredadevina06Pas encore d'évaluation
- Outcomes of COPDDocument6 pagesOutcomes of COPDRISKIPas encore d'évaluation
- Oxygen ToxicityDocument21 pagesOxygen ToxicityDonga DongoPas encore d'évaluation
- Oxygen InsufficiencyDocument70 pagesOxygen InsufficiencydaisyPas encore d'évaluation
- Asthma and COPDDocument28 pagesAsthma and COPDShoaib PatelPas encore d'évaluation
- Acute Respiratory Distress SyndromeDocument24 pagesAcute Respiratory Distress SyndromePooja ShashidharanPas encore d'évaluation
- Oxygen Therapy GuidelinesDocument19 pagesOxygen Therapy GuidelinesAyuna Rahmani0% (1)
- Formulas de PesoDocument4 pagesFormulas de PesoviaereaPas encore d'évaluation
- Combat Anesthesia - The First 24 Hours 1st Edition PDFDocument608 pagesCombat Anesthesia - The First 24 Hours 1st Edition PDFviaerea100% (1)
- Urgencias MetabolicasDocument11 pagesUrgencias MetabolicasviaereaPas encore d'évaluation
- Medical Education A History in 100 ImagesDocument236 pagesMedical Education A History in 100 ImagesviaereaPas encore d'évaluation
- PK of Drug OverdoseDocument32 pagesPK of Drug OverdoseviaereaPas encore d'évaluation
- Lactancia - Materna en MéxicoDocument21 pagesLactancia - Materna en MéxicoviaereaPas encore d'évaluation
- Crecimiento y Desarrollo PediaDocument369 pagesCrecimiento y Desarrollo PediaviaereaPas encore d'évaluation
- Transfusion in Trauma SCARE 2012Document6 pagesTransfusion in Trauma SCARE 2012viaereaPas encore d'évaluation
- Bleeding Is Out, Your Own Blood Is in 2014Document4 pagesBleeding Is Out, Your Own Blood Is in 2014viaereaPas encore d'évaluation
- ROBERTS Et Al 1988 AnaesthesiaDocument4 pagesROBERTS Et Al 1988 AnaesthesiaviaereaPas encore d'évaluation
- Massive Haemorrhage PPT en PDFDocument18 pagesMassive Haemorrhage PPT en PDFviaereaPas encore d'évaluation
- ATOTW 136 Major Haemorrhage Part 1 2009Document6 pagesATOTW 136 Major Haemorrhage Part 1 2009viaereaPas encore d'évaluation
- Physical Principles of Clinical Measurements 1966Document14 pagesPhysical Principles of Clinical Measurements 1966viaereaPas encore d'évaluation
- The Exam Will Be 25 Multiple Choice Questions Worth 2 Points EachDocument1 pageThe Exam Will Be 25 Multiple Choice Questions Worth 2 Points EachviaereaPas encore d'évaluation
- Rt-30 Pharm HW - Henry LeungDocument48 pagesRt-30 Pharm HW - Henry LeungviaereaPas encore d'évaluation
- Obtaining A AbgDocument1 pageObtaining A AbgviaereaPas encore d'évaluation
- Nitric Oxide Production and Signaling in InflammationDocument9 pagesNitric Oxide Production and Signaling in InflammationviaereaPas encore d'évaluation
- Catibayan Reflection AR VRDocument6 pagesCatibayan Reflection AR VRSheina Marie BariPas encore d'évaluation
- History of AIDocument27 pagesHistory of AImuzammalPas encore d'évaluation
- Diverse Narrative Structures in Contemporary Picturebooks: Opportunities For Children's Meaning-MakingDocument11 pagesDiverse Narrative Structures in Contemporary Picturebooks: Opportunities For Children's Meaning-MakingBlanca HernándezPas encore d'évaluation
- Mohd Ali 17: By:-Roll NoDocument12 pagesMohd Ali 17: By:-Roll NoMd AliPas encore d'évaluation
- CSL - Reflection Essay 1Document7 pagesCSL - Reflection Essay 1api-314849412Pas encore d'évaluation
- 10 Fonts For A Better WebsiteDocument3 pages10 Fonts For A Better WebsiteAlyzza Kara AcabalPas encore d'évaluation
- 2 Beginner 2nd GradeDocument12 pages2 Beginner 2nd GradesebPas encore d'évaluation
- Cambridge IGCSE: BIOLOGY 0610/31Document20 pagesCambridge IGCSE: BIOLOGY 0610/31Balachandran PalaniandyPas encore d'évaluation
- Creativity & Innovation Brainstorming TechniquesDocument50 pagesCreativity & Innovation Brainstorming TechniquesFirdhaus SakaffPas encore d'évaluation
- Detailed Lesson Plan in PED 12Document10 pagesDetailed Lesson Plan in PED 12alcomfeloPas encore d'évaluation
- 2016 01 15 12 00 22 PDFDocument26 pages2016 01 15 12 00 22 PDFABHIJEET SHARMAPas encore d'évaluation
- LDS Conference Report 1930 Semi AnnualDocument148 pagesLDS Conference Report 1930 Semi AnnualrjjburrowsPas encore d'évaluation
- TreeAgePro 2013 ManualDocument588 pagesTreeAgePro 2013 ManualChristian CifuentesPas encore d'évaluation
- Occupant Response To Vehicular VibrationDocument16 pagesOccupant Response To Vehicular VibrationAishhwarya Priya100% (1)
- Girl: Dad, I Need A Few Supplies For School, and I Was Wondering If - . .Document3 pagesGirl: Dad, I Need A Few Supplies For School, and I Was Wondering If - . .AKSHATPas encore d'évaluation
- Software Development Life CycleDocument70 pagesSoftware Development Life CycleChaitanya MalikPas encore d'évaluation
- Sta 305Document156 pagesSta 305mumbi makangaPas encore d'évaluation
- Final BasantDocument22 pagesFinal BasantMuqaddas IsrarPas encore d'évaluation
- Appraising The Secretaries of Sweet Water UniversityDocument4 pagesAppraising The Secretaries of Sweet Water UniversityZain4uPas encore d'évaluation
- Breast Cancer ChemotherapyDocument7 pagesBreast Cancer Chemotherapydini kusmaharaniPas encore d'évaluation
- Presente Progresive TenseDocument21 pagesPresente Progresive TenseAriana ChanganaquiPas encore d'évaluation
- ECON 4035 - Excel GuideDocument13 pagesECON 4035 - Excel GuideRosario Rivera NegrónPas encore d'évaluation
- The Acceptability of Indian Mango Leaves Powdered As A Tea: (Mangifera Indica Linn.)Document22 pagesThe Acceptability of Indian Mango Leaves Powdered As A Tea: (Mangifera Indica Linn.)Marissa M. DoriaPas encore d'évaluation
- Singular & Plural Nouns: Regular PluralsDocument4 pagesSingular & Plural Nouns: Regular PluralsМарина ВетерPas encore d'évaluation
- They Cried MonsterDocument13 pagesThey Cried MonstermassuroPas encore d'évaluation
- Fundamentals of Marketing Management: by Prabhat Ranjan Choudhury, Sr. Lecturer, B.J.B (A) College, BhubaneswarDocument53 pagesFundamentals of Marketing Management: by Prabhat Ranjan Choudhury, Sr. Lecturer, B.J.B (A) College, Bhubaneswarprabhatrc4235Pas encore d'évaluation
- MK Slide PDFDocument26 pagesMK Slide PDFPrabakaran NrdPas encore d'évaluation
- SiteVisit - Name (Done Excel, Pending CC)Document147 pagesSiteVisit - Name (Done Excel, Pending CC)CK AngPas encore d'évaluation
- Performance Task in Mathematics 10 First Quarter: GuidelinesDocument2 pagesPerformance Task in Mathematics 10 First Quarter: Guidelinesbelle cutiee100% (3)