Vous aimerez peut-être aussi
- 7 RespirationDocument15 pages7 RespirationCLEMENTPas encore d'évaluation
- 1.introduction To Physiology, The Cell and General PhysiologDocument3 pages1.introduction To Physiology, The Cell and General PhysiologCLEMENT100% (1)
- 8.aviation, Space and Deep Sea Diving PhysiologyDocument5 pages8.aviation, Space and Deep Sea Diving PhysiologyCLEMENTPas encore d'évaluation
- History Taking and Physical Examination, Level 5Document48 pagesHistory Taking and Physical Examination, Level 5CLEMENTPas encore d'évaluation
- Sports PhysiologyDocument3 pagesSports PhysiologyCLEMENTPas encore d'évaluation
- 2.membrane Physiology, Nerve and MuscleDocument6 pages2.membrane Physiology, Nerve and MuscleCLEMENT100% (1)
- Aqueous SolutionsDocument57 pagesAqueous SolutionsCLEMENTPas encore d'évaluation
- Synthesis of Eicosanoids and SignalingDocument10 pagesSynthesis of Eicosanoids and SignalingCLEMENTPas encore d'évaluation
- The HeartDocument15 pagesThe HeartCLEMENTPas encore d'évaluation
- Pathogenesis and Classification of NeoplasiaDocument36 pagesPathogenesis and Classification of NeoplasiaCLEMENT0% (1)
- Development of A Research ProposalDocument25 pagesDevelopment of A Research ProposalCLEMENTPas encore d'évaluation
- Clinical Epidemiology of The Leading Causes of MorbidityDocument22 pagesClinical Epidemiology of The Leading Causes of MorbidityCLEMENTPas encore d'évaluation
- Pathological Response To Infectious and Parasitic DiseasesDocument36 pagesPathological Response To Infectious and Parasitic DiseasesCLEMENTPas encore d'évaluation
- Nutritional and Nutritional RequirementsDocument25 pagesNutritional and Nutritional RequirementsCLEMENTPas encore d'évaluation
- Malaria: Definition: Infection Due To PlasmodiumDocument17 pagesMalaria: Definition: Infection Due To PlasmodiumCLEMENTPas encore d'évaluation
- Genetics: Definition: Branch of Biologic Science That Deals With Transmission of Characters From Parents To OffspringsDocument22 pagesGenetics: Definition: Branch of Biologic Science That Deals With Transmission of Characters From Parents To OffspringsCLEMENTPas encore d'évaluation
- Growth and Development in Children by Dr. Rafia. IqbalDocument34 pagesGrowth and Development in Children by Dr. Rafia. IqbalCLEMENTPas encore d'évaluation
- Clinical Use of Antimicrobial AgentsDocument24 pagesClinical Use of Antimicrobial AgentsCLEMENTPas encore d'évaluation
- DicDocument17 pagesDicCLEMENT0% (1)
- Gas Transport in Blood PPT 1Document34 pagesGas Transport in Blood PPT 1CLEMENTPas encore d'évaluation
- Antigens, Hapteins, Immunogens Lectures 10.1.06Document32 pagesAntigens, Hapteins, Immunogens Lectures 10.1.06CLEMENTPas encore d'évaluation
- Basic PathologyDocument37 pagesBasic PathologyCLEMENTPas encore d'évaluation
- Disorders of Skeletal, Cardiac and Smooth Muscle Cells-Myasthenia Gravis, Muscular Dystrophy and MyotoniaDocument51 pagesDisorders of Skeletal, Cardiac and Smooth Muscle Cells-Myasthenia Gravis, Muscular Dystrophy and MyotoniaCLEMENTPas encore d'évaluation
- Pain Sensation and Pathophysiology of Headache: Presenter: DR William Ramadhan.A FACILITATOR: DR M A. NjelekelaDocument34 pagesPain Sensation and Pathophysiology of Headache: Presenter: DR William Ramadhan.A FACILITATOR: DR M A. NjelekelaCLEMENTPas encore d'évaluation
- Genital UlcersDocument17 pagesGenital UlcersCLEMENTPas encore d'évaluation
- Cellular Growth, Injury and Adaptation: DR Kasonda Pediatrician 17/5/2017Document3 pagesCellular Growth, Injury and Adaptation: DR Kasonda Pediatrician 17/5/2017CLEMENTPas encore d'évaluation
- Protein Energy Malnutrition (PEM)Document39 pagesProtein Energy Malnutrition (PEM)CLEMENT100% (3)
- Hypertension: Definition: BP 95% Percentile Incidence: 1% of All AdolescentsDocument15 pagesHypertension: Definition: BP 95% Percentile Incidence: 1% of All AdolescentsCLEMENTPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Chicken Wing Dissection InstructionsDocument4 pagesChicken Wing Dissection InstructionsSandra Fowler100% (1)
- 2015 Wassce - Biology 2 SolutionDocument9 pages2015 Wassce - Biology 2 SolutionKelvin Yeboah TenkorangPas encore d'évaluation
- Latin For AnatomyDocument4 pagesLatin For AnatomyAchraf RabadiPas encore d'évaluation
- IGCSE Bio - Blood DonationDocument13 pagesIGCSE Bio - Blood DonationTroy CampbellPas encore d'évaluation
- Sensory and Motor Nerve EndingsDocument42 pagesSensory and Motor Nerve EndingsMark GanirPas encore d'évaluation
- Biomechanics Mid TermDocument49 pagesBiomechanics Mid TermSnehasis Routray100% (1)
- Dendrites Receive Electrochemical Impulses From Other NeuronsDocument3 pagesDendrites Receive Electrochemical Impulses From Other NeuronsJessa Mae IbalPas encore d'évaluation
- Intestinal NematodesDocument88 pagesIntestinal NematodesVincent Manganaan100% (1)
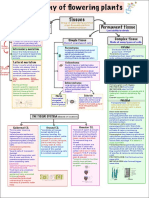
- Anatomy of Flowering Plants Mind MapDocument2 pagesAnatomy of Flowering Plants Mind MapAstha Agrawal100% (8)
- Cell AnalogyDocument11 pagesCell AnalogyMikaella Jayne CatanaoanPas encore d'évaluation
- 1 Endocrine System Review GuidemwDocument3 pages1 Endocrine System Review GuidemwdfgvsfdsfPas encore d'évaluation
- Cardiovascular QuestionDocument9 pagesCardiovascular Questionmedic99Pas encore d'évaluation
- Vertebrate Systems SummaryDocument29 pagesVertebrate Systems SummaryHazel Grace Bellen100% (1)
- 5 Chapter AnaphyDocument8 pages5 Chapter Anaphyjeanbecera19Pas encore d'évaluation
- Pitting and Non-Pitting Oedema: Clinical SkillsDocument3 pagesPitting and Non-Pitting Oedema: Clinical SkillsDinnar Ulya FauziahPas encore d'évaluation
- The Histopathological Approach To Inflammatory Bowel Disease: A Practice Guide.Document18 pagesThe Histopathological Approach To Inflammatory Bowel Disease: A Practice Guide.Ana CanastraPas encore d'évaluation
- Ceva NecropsyDocument18 pagesCeva NecropsyNanda Ayu Cindy KashiwabaraPas encore d'évaluation
- The - Skeletal - System Lab ActDocument13 pagesThe - Skeletal - System Lab Actwelfred indinoPas encore d'évaluation
- Cell Biology Practice 2Document15 pagesCell Biology Practice 2NgMinhHaiPas encore d'évaluation
- Autotrophic Nutrition Heterotrophic NutritionDocument1 pageAutotrophic Nutrition Heterotrophic NutritionAditya KediaPas encore d'évaluation
- Nervous System Mind MapDocument1 pageNervous System Mind MapAra Malagón González100% (1)
- Bio 12 Answer Key CH 8-14Document33 pagesBio 12 Answer Key CH 8-14api-2620290510% (1)
- Ascomycotina Class PPT 2014Document80 pagesAscomycotina Class PPT 2014Shaezarah Mohamudally67% (3)
- Marieb Ch11aDocument23 pagesMarieb Ch11aapi-229554503Pas encore d'évaluation
- Third Stage Complication of LabourDocument56 pagesThird Stage Complication of LabourshravaniPas encore d'évaluation
- Integrated Studies Grade 3 Term 1Document6 pagesIntegrated Studies Grade 3 Term 1Kimarley CampbellPas encore d'évaluation
- CBSE Class 11 Biology Chapter 21 Neural Control and Coordination NotesDocument7 pagesCBSE Class 11 Biology Chapter 21 Neural Control and Coordination NotesShivalgiri Goswami0% (1)
- Part of BodyDocument4 pagesPart of Bodyanon_535068952Pas encore d'évaluation
- Syllabus: 1.1.1 E, F, G, H & J: Homework: Revise All From Today For Your Test 1Document36 pagesSyllabus: 1.1.1 E, F, G, H & J: Homework: Revise All From Today For Your Test 1Nusrat'Felix' KhanPas encore d'évaluation
- The Mechanism of Respiration.Document12 pagesThe Mechanism of Respiration.Shimmering MoonPas encore d'évaluation