Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Elevator ControlDocument3 pagesElevator ControlNATHANPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
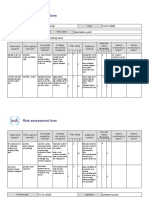
- Risk Assessment Project Iosh - MsDocument2 pagesRisk Assessment Project Iosh - MsSanjeev Kumar75% (32)
- ClassnotesonbasicDC DCconverters EP N4Document23 pagesClassnotesonbasicDC DCconverters EP N4Gerardo Treviño GarciaPas encore d'évaluation
- Helminths: NematodesDocument17 pagesHelminths: NematodesNicolle PanchoPas encore d'évaluation
- Drypix 6000 12eDocument501 pagesDrypix 6000 12eraj_meditech100% (1)
- D20 25 30 33S-5 D35C-5 (Sb1109e06) PDFDocument424 pagesD20 25 30 33S-5 D35C-5 (Sb1109e06) PDFGORD100% (8)
- Cryogenic Insulation TechnologyDocument61 pagesCryogenic Insulation Technologyeduard.turon100% (1)
- A Team - Group - ESG Handbook 2021 July 2021Document69 pagesA Team - Group - ESG Handbook 2021 July 2021Prajwala JankarPas encore d'évaluation
- Civil 416Document2 pagesCivil 416tskh11Pas encore d'évaluation
- 120Document349 pages120xdyj2005Pas encore d'évaluation
- Portable Load Banks: CressallDocument1 pagePortable Load Banks: CressallYashveer26Pas encore d'évaluation
- Lesson Plan 1 - Agriculture in Your LifeDocument6 pagesLesson Plan 1 - Agriculture in Your Lifeapi-235918896Pas encore d'évaluation
- Cengage Advantage Books Fundamentals of Business Law Excerpted Cases 3rd Edition Roger Leroy Miller Test BankDocument26 pagesCengage Advantage Books Fundamentals of Business Law Excerpted Cases 3rd Edition Roger Leroy Miller Test Bankladonnaaidanm5s100% (28)
- ABB Photovoltaic DisconnectorsDocument6 pagesABB Photovoltaic DisconnectorsBog PenPas encore d'évaluation
- Layout - Foundation Drawing - Air BlowerDocument2 pagesLayout - Foundation Drawing - Air BlowerBabel THIAMPas encore d'évaluation
- A Lightweight True Random Number Generator For Root of Trust ApplicationsDocument11 pagesA Lightweight True Random Number Generator For Root of Trust ApplicationsMADDULURI JAYASRIPas encore d'évaluation
- Fundamental and Technical Analysis of Iron and Steel SIP PROJECTDocument34 pagesFundamental and Technical Analysis of Iron and Steel SIP PROJECThaveuever910Pas encore d'évaluation
- 4 TH Sem UG Osmoregulation in Aquatic VertebratesDocument6 pages4 TH Sem UG Osmoregulation in Aquatic VertebratesBasak ShreyaPas encore d'évaluation
- Jurnal Semi FowlerDocument6 pagesJurnal Semi FowlerHartina RolobessyPas encore d'évaluation
- Semicounductors & Pn-Junction (Complete)Document47 pagesSemicounductors & Pn-Junction (Complete)Khalid AliPas encore d'évaluation
- 3rd Quarter Performance TaskDocument3 pages3rd Quarter Performance TaskJaime CrispinoPas encore d'évaluation
- DalmatiaDocument265 pagesDalmatiaomissam2Pas encore d'évaluation
- Comparison of Ozone Vs Uv in WaterDocument1 pageComparison of Ozone Vs Uv in WaterRajesh PandeyPas encore d'évaluation
- Revision For The First 1 English 8Document6 pagesRevision For The First 1 English 8hiidaxneee urrrmPas encore d'évaluation
- Hirschsprung's Disease - AthigamanDocument128 pagesHirschsprung's Disease - Athigamanprived100% (4)
- 3 Particle Nature of Matter PDFDocument4 pages3 Particle Nature of Matter PDFAtheer AlaniPas encore d'évaluation
- Geo-Technical Investigation On Black Cotton Soils: GeotechnicalinvestigationonblackcottonsoilsDocument5 pagesGeo-Technical Investigation On Black Cotton Soils: GeotechnicalinvestigationonblackcottonsoilsDevendrasinh PadhiyarPas encore d'évaluation
- TM TC For NanosatelliteDocument4 pagesTM TC For NanosatelliteSreeja SujithPas encore d'évaluation
- Divine Child International School, Adalaj Revision Worksheet Grade 6, Maths Choose The Correct OptionDocument2 pagesDivine Child International School, Adalaj Revision Worksheet Grade 6, Maths Choose The Correct OptionNatasha VidhaniPas encore d'évaluation
- CF1900SS-DF Example Spec - Rev1Document1 pageCF1900SS-DF Example Spec - Rev1parsiti unnesPas encore d'évaluation