Vous aimerez peut-être aussi
- Pulmo Kardio Gastro Hepato Logi Entero: Musculo Ginjal-HtDocument2 pagesPulmo Kardio Gastro Hepato Logi Entero: Musculo Ginjal-HtAnonymous QDjS3hyUPas encore d'évaluation
- A. Awkward Posture Tabel 4.2 Ergonomics Risk Factor: Awkward PostureDocument3 pagesA. Awkward Posture Tabel 4.2 Ergonomics Risk Factor: Awkward PostureAnonymous QDjS3hyUPas encore d'évaluation
- Lampiran 16. Media Edukasi Still PictureDocument1 pageLampiran 16. Media Edukasi Still PictureAnonymous QDjS3hyUPas encore d'évaluation
- Print - CA MammaeeDocument1 pagePrint - CA MammaeeAnonymous QDjS3hyUPas encore d'évaluation
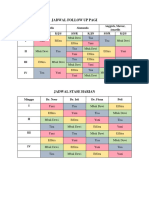
- Jadwal Follow Up Pagi: Minggu Dahlia Alamanda Anggrek, Mawar, Amarilis S/S/R K/J/S S/S/R K/J/S S/S/R K/J/S IDocument1 pageJadwal Follow Up Pagi: Minggu Dahlia Alamanda Anggrek, Mawar, Amarilis S/S/R K/J/S S/S/R K/J/S S/S/R K/J/S IAnonymous QDjS3hyUPas encore d'évaluation
- Dry Eye Disease 2Document6 pagesDry Eye Disease 2Anonymous QDjS3hyUPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Pathophysiology of Cardiogenic Pulmonary EdemaDocument13 pagesPathophysiology of Cardiogenic Pulmonary EdemaIrina DuceacPas encore d'évaluation
- Acute Decompensated HeartDocument7 pagesAcute Decompensated HeartRay MartínezPas encore d'évaluation
- Pathophysiology of Cardiogenic Pulmonary Edema - UpToDateDocument14 pagesPathophysiology of Cardiogenic Pulmonary Edema - UpToDateStefani AtllePas encore d'évaluation
- Acute Heart FailureDocument11 pagesAcute Heart FailureKhaireza KhairuddinPas encore d'évaluation
- Pathophysiology of Cardiogenic Pulmonary EdemaDocument8 pagesPathophysiology of Cardiogenic Pulmonary EdemaLili Fiorela CRPas encore d'évaluation
- Mitral Valve Prolapse (MVP) : Auscultation of MurmursDocument55 pagesMitral Valve Prolapse (MVP) : Auscultation of MurmursYagyeshPas encore d'évaluation
- August 9, 2006 Joann Lindenfeld, MDDocument60 pagesAugust 9, 2006 Joann Lindenfeld, MDkamel6Pas encore d'évaluation
- Management of Pulmonary Hypertension in the ICUDocument52 pagesManagement of Pulmonary Hypertension in the ICUsarsalPas encore d'évaluation
- Advor 2022Document11 pagesAdvor 2022Guilherme CarelliPas encore d'évaluation
- Congestive Heart Failure Guide: Causes, Symptoms, TreatmentsDocument64 pagesCongestive Heart Failure Guide: Causes, Symptoms, TreatmentsBentoys StreetPas encore d'évaluation
- Importance of Venous Congestion For Worsening of Renal Function in Advanced Decompensated Heart FailureDocument8 pagesImportance of Venous Congestion For Worsening of Renal Function in Advanced Decompensated Heart FailureRaul FernandoPas encore d'évaluation
- Aki NephrosapDocument82 pagesAki NephrosapMARCELO DE ROSA100% (1)
- Congestive Cardiac FailureDocument38 pagesCongestive Cardiac FailureSalman KhanPas encore d'évaluation
- Flash Pulmonary EdemaDocument11 pagesFlash Pulmonary EdemaEda SopPas encore d'évaluation
- European Heart Journal Review of Inotropic TherapiesDocument11 pagesEuropean Heart Journal Review of Inotropic TherapiesdubblewalkerPas encore d'évaluation
- Cardiorenal SyndromeDocument89 pagesCardiorenal SyndromeGabriyah HamzahPas encore d'évaluation
- Acute Cardiorenal Syndrome An UpdateDocument10 pagesAcute Cardiorenal Syndrome An UpdateErika Jiménez De LaraPas encore d'évaluation
- Causes and Treatment of Refractory Edema in Adults - UpToDateDocument28 pagesCauses and Treatment of Refractory Edema in Adults - UpToDateSuci WijayaPas encore d'évaluation
- ACUTE DECOMPENSATED HEART FAILUREDocument71 pagesACUTE DECOMPENSATED HEART FAILUREVivek Anandan100% (1)
- Uworld Notes CK PDFDocument123 pagesUworld Notes CK PDFNik KalairPas encore d'évaluation
- Heart Failure in ChildrenDocument9 pagesHeart Failure in ChildrenGustiTiballaPas encore d'évaluation
- Myocardial Infarction Covid Heart Failure Quiz RLE 5-6-2021Document58 pagesMyocardial Infarction Covid Heart Failure Quiz RLE 5-6-2021MuhyeeSalaIdjadPas encore d'évaluation
- ER & CCU ProtocolDocument14 pagesER & CCU ProtocolatinafansifPas encore d'évaluation
- Final Research PaperDocument16 pagesFinal Research Paperapi-593862121Pas encore d'évaluation
- Daftar Singkatan SMF JAntungDocument5 pagesDaftar Singkatan SMF JAntungBobby RahmantoPas encore d'évaluation
- Good BooksDocument16 pagesGood BooksFbihansip bancel100% (1)
- Heart FailureDocument1 pageHeart FailureCecil-An DalanonPas encore d'évaluation
- 65-Year-Old Man Chest Pain Diagnosis Acute Aortic DissectionDocument146 pages65-Year-Old Man Chest Pain Diagnosis Acute Aortic DissectionbbdddPas encore d'évaluation
- Treatment of Acute Decompensated Heart Failure - Components of TherapyDocument22 pagesTreatment of Acute Decompensated Heart Failure - Components of TherapyYahaira Borquez RiosPas encore d'évaluation