Vous aimerez peut-être aussi
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Management of Uterine Fibroid 2Document37 pagesManagement of Uterine Fibroid 2api-3705046100% (3)
- A Simple Guide to Adrenal Cancer, Diagnosis, Treatment and Related ConditionsD'EverandA Simple Guide to Adrenal Cancer, Diagnosis, Treatment and Related ConditionsPas encore d'évaluation
- Uterine FibroidsDocument21 pagesUterine FibroidsPrasun BiswasPas encore d'évaluation
- Uterinefibroids 130120064643 Phpapp02Document73 pagesUterinefibroids 130120064643 Phpapp02Tharun KumarPas encore d'évaluation
- Menstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoDocument36 pagesMenstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoAkinbani MoyosorePas encore d'évaluation
- Sakila MurmuDocument47 pagesSakila MurmuSakila murmuPas encore d'évaluation
- Malignant Tumors of Uterus: DR Tahira RizwanDocument52 pagesMalignant Tumors of Uterus: DR Tahira RizwanSadia YousafPas encore d'évaluation
- OSCE Revision OBG DocumentDocument60 pagesOSCE Revision OBG DocumentshreyaPas encore d'évaluation
- C SectionDocument50 pagesC SectionAlano S. LimgasPas encore d'évaluation
- Benign Gyecologic LesionDocument158 pagesBenign Gyecologic LesionArianne Joy C. TamarayPas encore d'évaluation
- Dr. Sharda Jain: Director: Secretary GeneralDocument91 pagesDr. Sharda Jain: Director: Secretary GeneraljijaniPas encore d'évaluation
- Uterine Fibroid-IzzatDocument20 pagesUterine Fibroid-IzzatcopperPas encore d'évaluation
- BENIGN OVARIAN DISEASES - Updated January 2018Document31 pagesBENIGN OVARIAN DISEASES - Updated January 2018daniel100% (1)
- Gynecological History Taking and ExaminationDocument17 pagesGynecological History Taking and Examinationnmsiswaridewi100% (1)
- 8surgical Management of Dysfunctional Uterine Bleeding - KabilanDocument14 pages8surgical Management of Dysfunctional Uterine Bleeding - KabilanNavani TharanPas encore d'évaluation
- Impey Obs and Gynae Revision Notes PDFDocument9 pagesImpey Obs and Gynae Revision Notes PDFRoisePas encore d'évaluation
- EUOGS OSCE Booklet 2020Document26 pagesEUOGS OSCE Booklet 2020Amanda Leow100% (1)
- Obstetric Gynaecology Jan 11Document32 pagesObstetric Gynaecology Jan 11selvie87Pas encore d'évaluation
- Uterus NeoDocument11 pagesUterus NeoHester Marie SimpiaPas encore d'évaluation
- O&G - Abnormal PresentationDocument32 pagesO&G - Abnormal PresentationAnironOrionPas encore d'évaluation
- Fetal Medicine - Bidyut KumarDocument4 pagesFetal Medicine - Bidyut KumarpatoxyzuPas encore d'évaluation
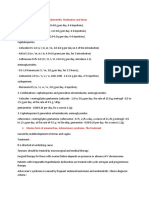
- Treatment of Acute Endometritis. Medication and DosesDocument3 pagesTreatment of Acute Endometritis. Medication and DosesTitoun LettounPas encore d'évaluation
- 11abnormal Uterine BleedingDocument32 pages11abnormal Uterine BleedingAkinbani MoyosorePas encore d'évaluation
- Assessment of Fetal Well BeingDocument46 pagesAssessment of Fetal Well BeingAumrin Fathima100% (1)
- Ca VulvaDocument38 pagesCa VulvavincentsharonPas encore d'évaluation
- Biomarkers in Abnormal Uterine Bleeding: Precision Medicine in Assisted Reproductive Technologies Special IssueDocument12 pagesBiomarkers in Abnormal Uterine Bleeding: Precision Medicine in Assisted Reproductive Technologies Special IssueWahyuning PutriPas encore d'évaluation
- OSCE Gynae-OSCE-MMSSDocument24 pagesOSCE Gynae-OSCE-MMSSMohammad Saifullah100% (1)
- Presented by DR - Shahbaz Ahmad Professor of Community MedicineDocument76 pagesPresented by DR - Shahbaz Ahmad Professor of Community MedicinePriya bhattiPas encore d'évaluation
- Ectopic Pregnancy5Document39 pagesEctopic Pregnancy5Muhammad AbeeshPas encore d'évaluation
- Early Pregnancy Problems: Presented byDocument28 pagesEarly Pregnancy Problems: Presented byMalk OmryPas encore d'évaluation
- Menorrhagia History Taking Notes 1Document2 pagesMenorrhagia History Taking Notes 1Shi Yi ChuaPas encore d'évaluation
- Hormonal ContraceptivesDocument25 pagesHormonal Contraceptivesmd easarur rahmanPas encore d'évaluation
- Ambulatory Hysteroscopy Evidence-Based Guide To Diagnosis and TherapyDocument23 pagesAmbulatory Hysteroscopy Evidence-Based Guide To Diagnosis and TherapyAngela EstevesPas encore d'évaluation
- Benign and Malignant Tumors of Female Genital TractDocument14 pagesBenign and Malignant Tumors of Female Genital TractDimitrios PapadopoulosPas encore d'évaluation
- Infertility: Reshmi SibyDocument80 pagesInfertility: Reshmi SibySusan ThomasPas encore d'évaluation
- Benign Disease of The UterusDocument27 pagesBenign Disease of The UterusnyangaraPas encore d'évaluation
- Printable - Thesis On Bishop ScoreDocument103 pagesPrintable - Thesis On Bishop Scoreanuaurv100% (3)
- Endometrial Hyperplasia: by Dr. Mervat AliDocument48 pagesEndometrial Hyperplasia: by Dr. Mervat AliAsh AmePas encore d'évaluation
- Laparoscopic Gynecologist Surgeon in HSR Layout BangaloreDocument8 pagesLaparoscopic Gynecologist Surgeon in HSR Layout BangaloreDr.Beena JeysinghPas encore d'évaluation
- InfertilityDocument14 pagesInfertilityDrChauhanPas encore d'évaluation
- Early Pregnancy Complications: Ectopic Pregnancy Gestational Trophoblastic Disease Ji Aggasid, JanniecelDocument60 pagesEarly Pregnancy Complications: Ectopic Pregnancy Gestational Trophoblastic Disease Ji Aggasid, JanniecelmedicoPas encore d'évaluation
- Menstrual Disorder and Abnormal BleedingDocument9 pagesMenstrual Disorder and Abnormal Bleedingdr_asalehPas encore d'évaluation
- Hysteroscopic Limitations PDFDocument59 pagesHysteroscopic Limitations PDFV R100% (1)
- Abnormal Uterine BleedingDocument5 pagesAbnormal Uterine Bleedingwuryan dewiPas encore d'évaluation
- (New) Early Pregnancy Complications RDocument51 pages(New) Early Pregnancy Complications RMesk Banat100% (2)
- Benign Lesions of Vulva and VaginaDocument34 pagesBenign Lesions of Vulva and VaginaCabdiPas encore d'évaluation
- Genital FistulaeDocument27 pagesGenital Fistulaeapi-3705046100% (1)
- د.عبد الزهره THE GYNAECOLOGICAL EXAMINATION-1 (Muhadharaty)Document29 pagesد.عبد الزهره THE GYNAECOLOGICAL EXAMINATION-1 (Muhadharaty)MohammedPas encore d'évaluation
- HysterosDocument17 pagesHysterosAnto PopaPas encore d'évaluation
- Myoma UteriDocument8 pagesMyoma UteriFaraida Arvilla100% (1)
- MenorrhagiaDocument4 pagesMenorrhagiaFlloyd_Martin__1259Pas encore d'évaluation
- Topic AmenorrheaDocument23 pagesTopic AmenorrheaMohammed AbdulPas encore d'évaluation
- Obs History Taking FormatDocument24 pagesObs History Taking FormatBibek PandeyPas encore d'évaluation
- Benign Gynecologic TumorsDocument57 pagesBenign Gynecologic TumorsDexter IanPas encore d'évaluation
- Cervical Intraepithelial Neoplasia and Cervical CancerDocument28 pagesCervical Intraepithelial Neoplasia and Cervical CancerNatnael100% (1)
- Ectopic Pregnancy: by Amielia Mazwa Rafidah Obstetric and Gynecology DepartmentDocument43 pagesEctopic Pregnancy: by Amielia Mazwa Rafidah Obstetric and Gynecology DepartmentAlrick AsentistaPas encore d'évaluation
- Dopplerinpregnancy 130823082426 Phpapp02Document64 pagesDopplerinpregnancy 130823082426 Phpapp02Herry SasukePas encore d'évaluation
- Uterus TransplantationDocument28 pagesUterus TransplantationJayaprakash SivamaniPas encore d'évaluation
- Obstetric Summm 1Document46 pagesObstetric Summm 1ملك عيسىPas encore d'évaluation
- Grade 10 Science - 2Document5 pagesGrade 10 Science - 2Nenia Claire Mondarte CruzPas encore d'évaluation
- What A Wonderful WorldDocument2 pagesWhat A Wonderful WorldDraganaPas encore d'évaluation
- 5 Point Scale PowerpointDocument40 pages5 Point Scale PowerpointMíchílín Ní Threasaigh100% (1)
- Neolms Week 1-2,2Document21 pagesNeolms Week 1-2,2Kimberly Quin CanasPas encore d'évaluation
- Chap6 Part1Document15 pagesChap6 Part1Francis Renjade Oafallas VinuyaPas encore d'évaluation
- Self Authoring SuiteDocument10 pagesSelf Authoring SuiteTanish Arora100% (3)
- Indiabix PDFDocument273 pagesIndiabix PDFMehedi Hasan ShuvoPas encore d'évaluation
- Music 10: 1 Quarterly Assessment (Mapeh 10 Written Work)Document4 pagesMusic 10: 1 Quarterly Assessment (Mapeh 10 Written Work)Kate Mary50% (2)
- Waldorf Curriculum ChartDocument1 pageWaldorf Curriculum Chartplanetalingua2020100% (1)
- Air Microbiology 2018 - IswDocument26 pagesAir Microbiology 2018 - IswOktalia Suci AnggraeniPas encore d'évaluation
- Tateni Home Care ServicesDocument2 pagesTateni Home Care ServicesAlejandro CardonaPas encore d'évaluation
- Quizo Yupanqui StoryDocument8 pagesQuizo Yupanqui StoryrickfrombrooklynPas encore d'évaluation
- DLL Week 7 MathDocument7 pagesDLL Week 7 MathMitchz TrinosPas encore d'évaluation
- Alankit Assignments LTD.: Project Report ONDocument84 pagesAlankit Assignments LTD.: Project Report ONmannuPas encore d'évaluation
- Vocabulary Inglés.Document14 pagesVocabulary Inglés.Psicoguía LatacungaPas encore d'évaluation
- Odisha Block Summary - NUAGAONDocument8 pagesOdisha Block Summary - NUAGAONRohith B.NPas encore d'évaluation
- G.R. No. 186450Document6 pagesG.R. No. 186450Jose Gonzalo SaldajenoPas encore d'évaluation
- PH Water On Stability PesticidesDocument6 pagesPH Water On Stability PesticidesMontoya AlidPas encore d'évaluation
- God's Word in Holy Citadel New Jerusalem" Monastery, Glodeni - Romania, Redactor Note. Translated by I.ADocument6 pagesGod's Word in Holy Citadel New Jerusalem" Monastery, Glodeni - Romania, Redactor Note. Translated by I.Abillydean_enPas encore d'évaluation
- Lunch Hour Meetings: Kiwanis Mission:: - Officers & Directors, 2018-2019Document2 pagesLunch Hour Meetings: Kiwanis Mission:: - Officers & Directors, 2018-2019Kiwanis Club of WaycrossPas encore d'évaluation
- Filipino Chicken Cordon BleuDocument7 pagesFilipino Chicken Cordon BleuHazel Castro Valentin-VillamorPas encore d'évaluation
- T2T - One - U12 - Grammarworksheet - 1 Should For Advice PDFDocument1 pageT2T - One - U12 - Grammarworksheet - 1 Should For Advice PDFGrissellPas encore d'évaluation
- Mbtruck Accessories BrochureDocument69 pagesMbtruck Accessories BrochureJoel AgbekponouPas encore d'évaluation
- IsaiahDocument7 pagesIsaiahJett Rovee Navarro100% (1)
- FFT SlidesDocument11 pagesFFT Slidessafu_117Pas encore d'évaluation
- Agitha Diva Winampi - Childhood MemoriesDocument2 pagesAgitha Diva Winampi - Childhood MemoriesAgitha Diva WinampiPas encore d'évaluation
- RPS Manajemen Keuangan IIDocument2 pagesRPS Manajemen Keuangan IIaulia endiniPas encore d'évaluation
- Pesticides 2015 - Full BookDocument297 pagesPesticides 2015 - Full BookTushar Savaliya100% (1)
- Industrial Cpmplus Enterprise Connectivity Collaborative Production ManagementDocument8 pagesIndustrial Cpmplus Enterprise Connectivity Collaborative Production ManagementEng Ahmad Bk AlbakheetPas encore d'évaluation
- Pudlo CWP TDS 2Document4 pagesPudlo CWP TDS 2azharPas encore d'évaluation