Vous aimerez peut-être aussi
- The Influence of Divorce On Children PDFDocument32 pagesThe Influence of Divorce On Children PDFMae Dacer100% (1)
- Risk Assessment - Installation of Exhaust FansDocument4 pagesRisk Assessment - Installation of Exhaust FansehteshamPas encore d'évaluation
- Understanding Psychoanalysis Understanding Movements in Modern ThoughtDocument241 pagesUnderstanding Psychoanalysis Understanding Movements in Modern Thoughtramiro_grivot100% (1)
- Mock Board Exam in Microbiology/ Virology/Mycology/ParasitologyDocument12 pagesMock Board Exam in Microbiology/ Virology/Mycology/ParasitologyShera Heart Go100% (1)
- Nebulization PRDocument8 pagesNebulization PRAmy LalringhluaniPas encore d'évaluation
- 8 Laws of Health: Streams of Light MinistryDocument9 pages8 Laws of Health: Streams of Light Ministryanjani kumarPas encore d'évaluation
- Bowel Wash and Flatus TubeDocument20 pagesBowel Wash and Flatus TubeBinal JoshiPas encore d'évaluation
- Nasogastric Tube Insertion 2006Document43 pagesNasogastric Tube Insertion 2006Fira W100% (1)
- Naso Gastric Tube FeedingDocument14 pagesNaso Gastric Tube FeedingSathya100% (2)
- Grastric Gavage & LavageDocument17 pagesGrastric Gavage & LavageJuliet Pua74% (19)
- Postnatal ExaminationDocument19 pagesPostnatal ExaminationAlpha100% (1)
- Tracheostomy Care: Presented by Sital B. Sharma M SC Nursing Student College of Nursing. N.B.M.C.HDocument74 pagesTracheostomy Care: Presented by Sital B. Sharma M SC Nursing Student College of Nursing. N.B.M.C.HShetal Sharma100% (1)
- Colostomy Care & IrrigationDocument18 pagesColostomy Care & Irrigationpbatongbakal100% (2)
- Procedure On Lumber PunctureDocument8 pagesProcedure On Lumber PunctureDimpal ChoudharyPas encore d'évaluation
- Past Papers:MICROBIOLOGYDocument6 pagesPast Papers:MICROBIOLOGYMalavikaN100% (3)
- Application of BindersDocument3 pagesApplication of BindersJayson Tom Briva Capaz100% (1)
- NG Tube FeedingDocument3 pagesNG Tube FeedingMaheswari BossPas encore d'évaluation
- SuctioningDocument5 pagesSuctioningNina Buenaventura100% (1)
- Care of The Hospitalized ChildDocument43 pagesCare of The Hospitalized ChildBinal Joshi50% (2)
- Activity Sheets7-8 (Using Appropriate Reading Style) W7-8Document7 pagesActivity Sheets7-8 (Using Appropriate Reading Style) W7-8Allan RemorozaPas encore d'évaluation
- Role of A Nurse in COVID-19 PandemicDocument6 pagesRole of A Nurse in COVID-19 PandemicMARYAM AL-KADHIM100% (3)
- Gastrostomy Tube Feeding ProcedureDocument2 pagesGastrostomy Tube Feeding Procedure浦船Pas encore d'évaluation
- Oxygen Therapy Administration For Paediatric PatientsDocument7 pagesOxygen Therapy Administration For Paediatric PatientsYwagar YwagarPas encore d'évaluation
- Administration of Nasogastric Tube FeedingDocument3 pagesAdministration of Nasogastric Tube FeedingAmy Lalringhluani Chhakchhuak100% (1)
- LBWDocument39 pagesLBWJOSLINPas encore d'évaluation
- Oral MedicationDocument11 pagesOral MedicationMayank KumarPas encore d'évaluation
- KMC FinalDocument36 pagesKMC FinalGandimarei100% (2)
- Baby BathDocument11 pagesBaby BathMayank Kumar100% (1)
- SHO Paper 2Document9 pagesSHO Paper 2Kenny Low100% (1)
- NGT FeedingDocument2 pagesNGT FeedingJD Escario100% (1)
- Tracheostomy Suctioning ProcedureDocument1 pageTracheostomy Suctioning ProcedurePearl DiBerardinoPas encore d'évaluation
- Procedure Steam Inhalation.Document10 pagesProcedure Steam Inhalation.PINKI DEBPas encore d'évaluation
- Nursing Preceptorship Re-Entry PlanDocument4 pagesNursing Preceptorship Re-Entry PlanMae DacerPas encore d'évaluation
- Care of New Born Basic Care of Normal NeonatesDocument4 pagesCare of New Born Basic Care of Normal NeonatesSREEDEVI T SURESHPas encore d'évaluation
- Suctioning 160714115618Document18 pagesSuctioning 160714115618jothi100% (1)
- Nasogastric Tube FeedingDocument7 pagesNasogastric Tube FeedingVina Empiales100% (1)
- Lesson Plan On Expressed Breast MilkDocument13 pagesLesson Plan On Expressed Breast MilkBinal Joshi100% (3)
- Teaching Learning Guide (Assist and NGT Insertion)Document12 pagesTeaching Learning Guide (Assist and NGT Insertion)BeanncaAngeles100% (1)
- Nursing Care of The Child Undergoing A TonsillectomyDocument2 pagesNursing Care of The Child Undergoing A Tonsillectomykelsey0% (1)
- Checklist For Chest PhysiotherapyDocument2 pagesChecklist For Chest PhysiotherapyCheran DeviPas encore d'évaluation
- Acute Biologic Crisis - FinalsDocument307 pagesAcute Biologic Crisis - FinalsMae DacerPas encore d'évaluation
- Modern Concept of Child CareDocument14 pagesModern Concept of Child CareKiranPas encore d'évaluation
- Skill 11 (1) ..Collection of Stool SpecimenDocument1 pageSkill 11 (1) ..Collection of Stool SpecimennetsquadPas encore d'évaluation
- Babybath 160831043204Document32 pagesBabybath 160831043204Glads D. Ferrer-JimlanoPas encore d'évaluation
- Oropharyngeal and Nasopharyngeal SuctioningDocument2 pagesOropharyngeal and Nasopharyngeal SuctioningAlana Caballero100% (1)
- Section P - Group 1 E.C.S. - Pediatric Ward Mr. Ralph P. Pilapil, R.N. Clinical InstructorDocument62 pagesSection P - Group 1 E.C.S. - Pediatric Ward Mr. Ralph P. Pilapil, R.N. Clinical InstructorClaudine N SantillanPas encore d'évaluation
- NG TubeDocument3 pagesNG TubeKenny JosefPas encore d'évaluation
- Foot and Hand Care: Learning ObjectivesDocument7 pagesFoot and Hand Care: Learning ObjectivesNITHYAPREMINI100% (1)
- Care of Chest Drainage: Articles RationaleDocument7 pagesCare of Chest Drainage: Articles Rationalepreeti sharmaPas encore d'évaluation
- Artificial or Supplimentary FoodDocument4 pagesArtificial or Supplimentary FoodArchana Sahu100% (1)
- Group 11 Cleft Lip and Cleft Palate Case Study N2BDocument46 pagesGroup 11 Cleft Lip and Cleft Palate Case Study N2BLerma PagcaliwanganPas encore d'évaluation
- Stomal TherapyDocument2 pagesStomal Therapyসায়ন্তন দত্ত100% (1)
- Artificial FeedingDocument7 pagesArtificial FeedingBRUELIN MELSHIA MPas encore d'évaluation
- NCP - Pediatrics Case Study (Pnuemonia With Down Syndrome)Document4 pagesNCP - Pediatrics Case Study (Pnuemonia With Down Syndrome)Charley DegamoPas encore d'évaluation
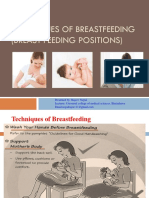
- Technique of Breast Feeding (Position of Breast Feeding)Document17 pagesTechnique of Breast Feeding (Position of Breast Feeding)Rajeev NepalPas encore d'évaluation
- Cleft Lip and Cleft PalateDocument16 pagesCleft Lip and Cleft Palatemacuka08100% (3)
- Gastric LavageDocument13 pagesGastric Lavagetibinj67Pas encore d'évaluation
- Procedure Checklist Chapter 27: Inserting An Indwelling Urinary Catheter (Male)Document4 pagesProcedure Checklist Chapter 27: Inserting An Indwelling Urinary Catheter (Male)jths100% (1)
- Post Mastectomy ExerciseDocument4 pagesPost Mastectomy ExerciseKusum RoyPas encore d'évaluation
- Gastrostomy Feeding ProcedureDocument5 pagesGastrostomy Feeding ProcedureRohini RaiPas encore d'évaluation
- Nasogastric Feeding or Gavage FeedingDocument47 pagesNasogastric Feeding or Gavage FeedingDr. Jayesh Patidar100% (1)
- Nebulizer ProcedureDocument2 pagesNebulizer Procedureralph_gailPas encore d'évaluation
- Case Management of Ari at PHC LevelDocument29 pagesCase Management of Ari at PHC Levelapi-3823785Pas encore d'évaluation
- Oxygen InhalationDocument32 pagesOxygen Inhalationvarshasharma05100% (3)
- Diarrhea CPDocument8 pagesDiarrhea CPAsma SaleemPas encore d'évaluation
- Applying An Icecap or Ice CollarDocument1 pageApplying An Icecap or Ice CollarAparna KinginiPas encore d'évaluation
- BedpanDocument14 pagesBedpanCarissa De Luzuriaga-Balaria100% (1)
- Baby-Friendly Hospital Initiative: R Dh@ker, Asst. Professor, RCNDocument32 pagesBaby-Friendly Hospital Initiative: R Dh@ker, Asst. Professor, RCNArchanaPas encore d'évaluation
- Urine Specimen Collection Procedure PDFDocument3 pagesUrine Specimen Collection Procedure PDFtincho9Pas encore d'évaluation
- Tepid-Sponging Check ListDocument1 pageTepid-Sponging Check ListSumi100% (2)
- Controlling Bleeding4AGastricGavage PDFDocument25 pagesControlling Bleeding4AGastricGavage PDFSam VeraPas encore d'évaluation
- NCM 417 - Midterm Exam 2016Document6 pagesNCM 417 - Midterm Exam 2016Mae DacerPas encore d'évaluation
- Acute Biologic Crisis - Finals 1Document127 pagesAcute Biologic Crisis - Finals 1Mae DacerPas encore d'évaluation
- NCM 417 - Final Exam 2015Document12 pagesNCM 417 - Final Exam 2015Mae DacerPas encore d'évaluation
- NCM 417 - Midterm Exam 2015Document6 pagesNCM 417 - Midterm Exam 2015Mae DacerPas encore d'évaluation
- Attendance Sheet Dec12Document2 pagesAttendance Sheet Dec12Mae DacerPas encore d'évaluation
- Exposed To Answering Different Tools in Critical Care Like GCSDocument3 pagesExposed To Answering Different Tools in Critical Care Like GCSMae DacerPas encore d'évaluation
- FNCP 2Document3 pagesFNCP 2Mae DacerPas encore d'évaluation
- Competency Appraisal: Summative AssessmentDocument14 pagesCompetency Appraisal: Summative AssessmentMae DacerPas encore d'évaluation
- NCM 417 - Final Exam 2014Document12 pagesNCM 417 - Final Exam 2014Mae DacerPas encore d'évaluation
- NCM 417 - Midterm Exam 2015Document5 pagesNCM 417 - Midterm Exam 2015Mae DacerPas encore d'évaluation
- The Living Legacy of San Juanico Bridge Chapter 3Document8 pagesThe Living Legacy of San Juanico Bridge Chapter 3Mae DacerPas encore d'évaluation
- Oral Revalida - NCM 417 2014 MidtermDocument10 pagesOral Revalida - NCM 417 2014 MidtermMae DacerPas encore d'évaluation
- Application LetterDocument5 pagesApplication LetterMae DacerPas encore d'évaluation
- RequirementsDocument3 pagesRequirementsMae DacerPas encore d'évaluation
- VII. TRAINING PROGRAMS (Start From The Most Recent Training.)Document4 pagesVII. TRAINING PROGRAMS (Start From The Most Recent Training.)Mae DacerPas encore d'évaluation
- Application Letter SampleDocument1 pageApplication Letter SampleMae Dacer100% (1)
- Annex Xiii Id Application FormDocument1 pageAnnex Xiii Id Application FormMae DacerPas encore d'évaluation
- Performance Task #1: Law of ExponentsDocument3 pagesPerformance Task #1: Law of ExponentsMae DacerPas encore d'évaluation
- Mobuzz Dengue AppDocument10 pagesMobuzz Dengue AppMae DacerPas encore d'évaluation
- Cover Page On ChecklistDocument15 pagesCover Page On ChecklistMae DacerPas encore d'évaluation
- Application For Oral DefenseDocument2 pagesApplication For Oral DefenseMae DacerPas encore d'évaluation
- Cathedral School of La NavalDocument3 pagesCathedral School of La NavalMae DacerPas encore d'évaluation
- The Phenomenon Itself As It Reveals Itself. This Open Approach AllowsDocument4 pagesThe Phenomenon Itself As It Reveals Itself. This Open Approach AllowsMae DacerPas encore d'évaluation
- 5 e Study NursingDocument9 pages5 e Study NursingMae DacerPas encore d'évaluation
- E-Learning in NursingDocument6 pagesE-Learning in NursingMae DacerPas encore d'évaluation
- Module Cancer Sample 1Document44 pagesModule Cancer Sample 1Mae DacerPas encore d'évaluation
- Cover Compliance AudirDocument1 pageCover Compliance AudirMae DacerPas encore d'évaluation
- NCP Step 1: Nutrition Assessment: SnapshotDocument2 pagesNCP Step 1: Nutrition Assessment: SnapshotBushra KainaatPas encore d'évaluation
- KKU MPH Research Papers 2017Document455 pagesKKU MPH Research Papers 2017Myo Tin Ko OoPas encore d'évaluation
- Zee Bedside ExamDocument20 pagesZee Bedside Examhikmat sheraniPas encore d'évaluation
- Pediatrics: by DR - Mohammad Z. Abu Sheikha@Document98 pagesPediatrics: by DR - Mohammad Z. Abu Sheikha@Mohamed AbbasPas encore d'évaluation
- Sample I-Search Paper: Living With AsthmaDocument7 pagesSample I-Search Paper: Living With AsthmaputriPas encore d'évaluation
- Student Tracking SystemDocument2 pagesStudent Tracking SystemCynthia LuayPas encore d'évaluation
- Ayad Et Al - Antibacterial.efficiency - PomeloDocument5 pagesAyad Et Al - Antibacterial.efficiency - PomeloJesus NavaPas encore d'évaluation
- Tropical Veterinary Science: Ready Today For TomorrowDocument8 pagesTropical Veterinary Science: Ready Today For TomorrowEsdinawan Carakantara SatrijaPas encore d'évaluation
- Tanaman HerbalDocument134 pagesTanaman Herbalwhy_smart03Pas encore d'évaluation
- RhabdomyolysisDocument4 pagesRhabdomyolysisEyz PabloPas encore d'évaluation
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateDocument18 pagesDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDatePaloma GBPas encore d'évaluation
- Updated NCCN Guidelines For Cervical Cancer.22Document2 pagesUpdated NCCN Guidelines For Cervical Cancer.22Hari NugrohoPas encore d'évaluation
- Energy Balance WorksheetDocument3 pagesEnergy Balance Worksheetsara wilsonPas encore d'évaluation
- Nursing Care of A Child Undergoing Diagnostic Techniques and OtherDocument12 pagesNursing Care of A Child Undergoing Diagnostic Techniques and OtherGenry TanPas encore d'évaluation
- Kasus Psi TraumaDocument17 pagesKasus Psi TraumaWulanPas encore d'évaluation
- 5. Chronic pancreatitis. СholelithiasisDocument58 pages5. Chronic pancreatitis. Сholelithiasischai rinPas encore d'évaluation
- OB Ward Case StudyDocument20 pagesOB Ward Case StudyIvan A. EleginoPas encore d'évaluation
- 05 23 12+Grad+Entire+IssueDocument48 pages05 23 12+Grad+Entire+IssueVivek SarthiPas encore d'évaluation
- DW - SRX - Optex High Complexity Epidemic Mathematical ModelingDocument1 pageDW - SRX - Optex High Complexity Epidemic Mathematical ModelingJuan Carlos RodriguezPas encore d'évaluation
- PPH Marking Key Boas Bwale RN, RMDocument6 pagesPPH Marking Key Boas Bwale RN, RMFan EliPas encore d'évaluation
- SARS: The Inside Story: Where Did SARS Come From?Document6 pagesSARS: The Inside Story: Where Did SARS Come From?ZauzaPas encore d'évaluation
- Latihan Abbreviation 2Document2 pagesLatihan Abbreviation 2Sherly AmeliaPas encore d'évaluation