Vous aimerez peut-être aussi
- 17 Use Cases For Graph Databases and Graph AnalyticsDocument24 pages17 Use Cases For Graph Databases and Graph Analyticsnoto susantoPas encore d'évaluation
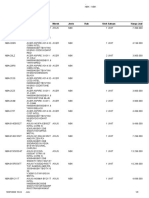
- Komdisc-Store: Kode Item Nama Item Jenis Rak Stok Harga Jual Satuan MerekDocument3 pagesKomdisc-Store: Kode Item Nama Item Jenis Rak Stok Harga Jual Satuan Mereknoto susantoPas encore d'évaluation
- DJI+Assistant+2+Release+Notes (1 2 5)Document29 pagesDJI+Assistant+2+Release+Notes (1 2 5)noto susantoPas encore d'évaluation
- JADWAL RETENSI-compressed PDFDocument118 pagesJADWAL RETENSI-compressed PDFnoto susanto100% (1)
- Social Media ButtonDocument1 pageSocial Media Buttonnoto susantoPas encore d'évaluation
- Medical Records 35-02-004: Policy StatementDocument6 pagesMedical Records 35-02-004: Policy Statementnoto susantoPas encore d'évaluation
- Medical Records Format - Riverside SBHC WVADocument4 pagesMedical Records Format - Riverside SBHC WVAnoto susantoPas encore d'évaluation
- Endocrine PathologyDocument157 pagesEndocrine Pathologynoto susantoPas encore d'évaluation
- Who MSD Mer 17.6 EngDocument656 pagesWho MSD Mer 17.6 Engnoto susantoPas encore d'évaluation
- Epinephrine 151218145527Document8 pagesEpinephrine 151218145527noto susanto100% (1)
- Incisionvsexcisionvsresection 140319203037 Phpapp02Document8 pagesIncisionvsexcisionvsresection 140319203037 Phpapp02noto susanto100% (1)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Kebo116 PDFDocument13 pagesKebo116 PDFbashraaPas encore d'évaluation
- Body Fluid DistributionDocument56 pagesBody Fluid DistributionZoya Morani100% (1)
- Immunosero ReviwerDocument73 pagesImmunosero ReviwerDarla YsavelPas encore d'évaluation
- Blood Bank Notes: History: de Motu Cordis Paved The Way For An Entirely New Arena ofDocument3 pagesBlood Bank Notes: History: de Motu Cordis Paved The Way For An Entirely New Arena ofRojane Camille A. ValdozPas encore d'évaluation
- Important Features Are: History of Neck SwellingsDocument4 pagesImportant Features Are: History of Neck SwellingsMuqtadir “The Ruler” Kuchiki100% (1)
- Spider Key - BiologyDocument3 pagesSpider Key - BiologyMartín EcheverriaPas encore d'évaluation
- Hematology Lecture Notes PDFDocument102 pagesHematology Lecture Notes PDFMarisa IzzaPas encore d'évaluation
- Biomecânica Do Músculo Esquelético PDFDocument24 pagesBiomecânica Do Músculo Esquelético PDFThiago LealPas encore d'évaluation
- GD in PregnancyDocument37 pagesGD in Pregnancymohammed makkiPas encore d'évaluation
- Periodontal Pocket and Bone Loss: Dr. Saima Akram Butt Department of PeriodontologyDocument25 pagesPeriodontal Pocket and Bone Loss: Dr. Saima Akram Butt Department of PeriodontologyAmit KumarPas encore d'évaluation
- Weetman-Immunology - of - PregnancyDocument4 pagesWeetman-Immunology - of - PregnancyPaul Alwin KhomanPas encore d'évaluation
- Interior Root WordsDocument3 pagesInterior Root WordsPaula McAuliffePas encore d'évaluation
- 5h-7-Thomas Lee Research Report Final March 2014Document3 pages5h-7-Thomas Lee Research Report Final March 2014api-251921674Pas encore d'évaluation
- VICTORIA MARTENS AUTOPSY REPORT - Sensitive ContentDocument31 pagesVICTORIA MARTENS AUTOPSY REPORT - Sensitive ContentCourtOnCamera100% (3)
- Central Nervous SystemDocument16 pagesCentral Nervous SystemafrinkhanPas encore d'évaluation
- 030722the Physiology of MicturitionDocument3 pages030722the Physiology of MicturitionAnnizah Paramitha100% (1)
- Laporan IKM KSM PK FEBRUARI 2022Document27 pagesLaporan IKM KSM PK FEBRUARI 2022Nur iffahPas encore d'évaluation
- PDFDocument570 pagesPDFEshaal FatimaPas encore d'évaluation
- Chap 5 ShortDocument43 pagesChap 5 Shortsheikh muhammad mubashirPas encore d'évaluation
- Dáp An AvDocument32 pagesDáp An AvDũngNguyễnHữu100% (1)
- ABDOMEN124Document25 pagesABDOMEN124Ashraf Alamin AhmedPas encore d'évaluation
- Penerapan Biomekanika, Respons Dan Adaptasi Otot RangkaDocument36 pagesPenerapan Biomekanika, Respons Dan Adaptasi Otot RangkaMohamad Rendy Firdianto100% (1)
- Blood Type Review WorksheetDocument2 pagesBlood Type Review WorksheetSofa100% (2)
- 4 - HUROPATH Atlas FNA - 2106Document9 pages4 - HUROPATH Atlas FNA - 2106Trần Thanh ViệnPas encore d'évaluation
- DLP in Science 3 - 4 Q2 WK 1 ValidatedDocument14 pagesDLP in Science 3 - 4 Q2 WK 1 ValidatedSalve Serrano100% (4)
- Nervous System Review Answer KeyDocument18 pagesNervous System Review Answer Keydanieljohnarboleda67% (3)
- Locomation and MovementDocument11 pagesLocomation and MovementsuryababaPas encore d'évaluation
- Physiotherapy in Pediatrics - NEURO MUSCULAR CONDITIONSDocument28 pagesPhysiotherapy in Pediatrics - NEURO MUSCULAR CONDITIONSKumar G PalaniPas encore d'évaluation
- Congenital Anomalies of Ureter BladderDocument17 pagesCongenital Anomalies of Ureter BladderAfiq SabriPas encore d'évaluation
- Chapter 20 HomeostasisDocument8 pagesChapter 20 HomeostasisLisa AllisyaPas encore d'évaluation