Vous aimerez peut-être aussi
- Pola Kelainan Tiroid Di RSUP Prof. Dr. R. D. Kandou Manado Periode Januari 2013 - Desember 2015Document8 pagesPola Kelainan Tiroid Di RSUP Prof. Dr. R. D. Kandou Manado Periode Januari 2013 - Desember 2015Bangun Said SantosoPas encore d'évaluation
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- SNNTDocument5 pagesSNNTBangun Said SantosoPas encore d'évaluation
- Pola Kelainan Tiroid Di RSUP Prof. Dr. R. D. Kandou Manado Periode Januari 2013 - Desember 2015Document8 pagesPola Kelainan Tiroid Di RSUP Prof. Dr. R. D. Kandou Manado Periode Januari 2013 - Desember 2015Bangun Said SantosoPas encore d'évaluation
- Android Game Programming by Example: Chapter 1: Player 1 UPDocument51 pagesAndroid Game Programming by Example: Chapter 1: Player 1 UPBangun Said SantosoPas encore d'évaluation
- IndexDocument13 pagesIndexBangun Said SantosoPas encore d'évaluation
- Lumbar Spondylosis: Clinical Presentation and Treatment ApproachesDocument12 pagesLumbar Spondylosis: Clinical Presentation and Treatment Approachesfreska ayu wardhaniPas encore d'évaluation
- DHF Dan HemofiliDocument3 pagesDHF Dan HemofiliBangun Said SantosoPas encore d'évaluation
- Dengue Fever in A Patient With SevereDocument11 pagesDengue Fever in A Patient With SevereBangun Said SantosoPas encore d'évaluation
- Handbook of Pediatric Eye and Systemic Disease PDFDocument650 pagesHandbook of Pediatric Eye and Systemic Disease PDFBangun Said SantosoPas encore d'évaluation
- CHFDocument17 pagesCHFBangun Said SantosoPas encore d'évaluation
- Wasabi Menu WEBDocument12 pagesWasabi Menu WEBBangun Said SantosoPas encore d'évaluation
- 3 CPR 1Document42 pages3 CPR 1Bangun Said SantosoPas encore d'évaluation
- Ophthalmology Survival Guide MapDocument78 pagesOphthalmology Survival Guide MapBangun Said SantosoPas encore d'évaluation
- Android Game Programming by Example: Chapter 1: Player 1 UPDocument51 pagesAndroid Game Programming by Example: Chapter 1: Player 1 UPBangun Said SantosoPas encore d'évaluation
- 8d6n Japan Alpine Route New DesignDocument2 pages8d6n Japan Alpine Route New DesignBangun Said SantosoPas encore d'évaluation
- Perspective: New England Journal MedicineDocument3 pagesPerspective: New England Journal MedicineBangun Said SantosoPas encore d'évaluation
- Vbac Royal CollegDocument31 pagesVbac Royal CollegBangun Said Santoso100% (1)
- Zika MeningoensefalitisDocument4 pagesZika MeningoensefalitisBangun Said SantosoPas encore d'évaluation
- Zika Virus: Review ArticleDocument12 pagesZika Virus: Review ArticleBangun Said SantosoPas encore d'évaluation
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Zika Virus Infection With Prolonged MaternalDocument10 pagesZika Virus Infection With Prolonged MaternalAtgy Dhita AnggraeniPas encore d'évaluation
- Zika1 With MicrocephalyDocument8 pagesZika1 With MicrocephalyBangun Said SantosoPas encore d'évaluation
- Handbook: For Clinical Management of DengueDocument124 pagesHandbook: For Clinical Management of DengueraattaiPas encore d'évaluation
- Handbook: For Clinical Management of DengueDocument124 pagesHandbook: For Clinical Management of DengueraattaiPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Seminar: Annelies Wilder-Smith, Eng-Eong Ooi, Olaf Horstick, Bridget WillsDocument14 pagesSeminar: Annelies Wilder-Smith, Eng-Eong Ooi, Olaf Horstick, Bridget WillsAlexander ArguelloPas encore d'évaluation
- HEALTH EDUCATION - GroupB - 2BDocument3 pagesHEALTH EDUCATION - GroupB - 2BKyle FernandezPas encore d'évaluation
- ABSTRACT-32nd World Congress of Internal Medicine 2014Document1 pageABSTRACT-32nd World Congress of Internal Medicine 2014Tenri AshariPas encore d'évaluation
- Dengue Fever in ChildrenDocument10 pagesDengue Fever in ChildrenMuhammad NajihPas encore d'évaluation
- Communicable Disease Nursing 2020Document421 pagesCommunicable Disease Nursing 2020Kenneth Myro GarciaPas encore d'évaluation
- Assess The Knowledge and Attitude On Prevention of Dengue Among The Patients AttendantsDocument6 pagesAssess The Knowledge and Attitude On Prevention of Dengue Among The Patients AttendantsIJAR JOURNALPas encore d'évaluation
- Nursing Students Learn About Infectious Disease EmergenciesDocument8 pagesNursing Students Learn About Infectious Disease EmergenciesNiceniadas CaraballePas encore d'évaluation
- Cashew Shell Extracts Kill Dengue Mosquito LarvaeDocument5 pagesCashew Shell Extracts Kill Dengue Mosquito LarvaeVernice OrtegaPas encore d'évaluation
- Internal Medicine Question Papers For MBBS Final Year StudentsDocument17 pagesInternal Medicine Question Papers For MBBS Final Year Studentsprinceej88% (8)
- Mosquito Repellent From Thai Essential Oils Against Dengue Fever Mosquito (Aedes Aegypti (L.) ) and Filarial Mosquito Vector (Culex Quinquefasciatus (Say) )Document6 pagesMosquito Repellent From Thai Essential Oils Against Dengue Fever Mosquito (Aedes Aegypti (L.) ) and Filarial Mosquito Vector (Culex Quinquefasciatus (Say) )Grilhamon ShenPas encore d'évaluation
- Dengue Prevention Health Teaching 09-16-10Document3 pagesDengue Prevention Health Teaching 09-16-10Bakushido100% (2)
- National Health Programmes in IndiaDocument8 pagesNational Health Programmes in IndiaRohit SharmaPas encore d'évaluation
- IMCI Guide for Assessing and Classifying Child with FeverDocument4 pagesIMCI Guide for Assessing and Classifying Child with FeverMariah Jane TaladuaPas encore d'évaluation
- Kathyrene B. BaylonDocument16 pagesKathyrene B. BaylonTata Duero LachicaPas encore d'évaluation
- Casumpang V. Cortejo G.R. No. 171127 - March 11, 2015 FactsDocument1 pageCasumpang V. Cortejo G.R. No. 171127 - March 11, 2015 FactsjaymeebqPas encore d'évaluation
- 6578 19694 2 PBDocument7 pages6578 19694 2 PBMark Nelson MagnoPas encore d'évaluation
- Test Result Normal Range Interpreta Tion Implicatio NDocument11 pagesTest Result Normal Range Interpreta Tion Implicatio NSitty Aizah MangotaraPas encore d'évaluation
- AdconDocument25 pagesAdconAnna AlcantaraPas encore d'évaluation
- Communicable Diseases 2.4-5.22Document9 pagesCommunicable Diseases 2.4-5.22Vhince PiscoPas encore d'évaluation
- Rice Genome ProjectDocument20 pagesRice Genome ProjectRanjith MuralidharanPas encore d'évaluation
- Term Paper Tungkol Sa DengueDocument5 pagesTerm Paper Tungkol Sa Dengueaflsikxgf100% (1)
- Medicine Nos.: Index Respiratory Problems Problem PG Problem PGDocument8 pagesMedicine Nos.: Index Respiratory Problems Problem PG Problem PGSamhitaPas encore d'évaluation
- Boy With Fever Has Malaria and ThalassemiaDocument1 pageBoy With Fever Has Malaria and ThalassemiaNashrah HusnaPas encore d'évaluation
- Prof. DR. Dr. Soeharyo Hadisaputro, SP - PD-KPTI-Dengue Infection in SepsisDocument42 pagesProf. DR. Dr. Soeharyo Hadisaputro, SP - PD-KPTI-Dengue Infection in SepsisOlivia DwimaswastiPas encore d'évaluation
- Proteinuria During Dengue Fever In: ChildrenDocument13 pagesProteinuria During Dengue Fever In: ChildrenSameeh MohPas encore d'évaluation
- Zika Virus Public HealthDocument2 pagesZika Virus Public Healthdianakusmi16051995Pas encore d'évaluation
- Management Severe DengueDocument18 pagesManagement Severe DengueMuhammad Fhandeka IsrarPas encore d'évaluation
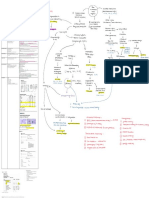
- Diagnosis of Dengue: Dr.M.sravana Durga, 1 Year Junior Resident MD PaediatricsDocument24 pagesDiagnosis of Dengue: Dr.M.sravana Durga, 1 Year Junior Resident MD PaediatricsAneesh MyneniPas encore d'évaluation
- CPG Dengue Infection PDF FinalDocument82 pagesCPG Dengue Infection PDF FinalTIong Tung WeiPas encore d'évaluation
- Dengue Fever Case StudyDocument55 pagesDengue Fever Case StudyGlory Holmes67% (6)