Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Ayurvedic Treatment of Enlarged Prostate GlandDocument28 pagesAyurvedic Treatment of Enlarged Prostate GlandRajeshKizziPas encore d'évaluation
- Blaylock Food0713 109Document13 pagesBlaylock Food0713 109ashatav3761100% (1)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- (K4) Male Reproductive SystemDocument73 pages(K4) Male Reproductive SystemJane Andrea Christiano DjianzoniePas encore d'évaluation
- Utmc - Utoledo.edu Depts Nursing Pdfs Basic EKG RefresherDocument210 pagesUtmc - Utoledo.edu Depts Nursing Pdfs Basic EKG RefresherTrish HồPas encore d'évaluation
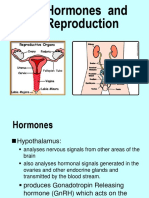
- Hormones and the Reproductive System ExplainedDocument24 pagesHormones and the Reproductive System ExplainedJane Andrea Christiano DjianzoniePas encore d'évaluation
- Discharge Planning and NCP SDocument8 pagesDischarge Planning and NCP SRainier RamosPas encore d'évaluation
- Basal Cell Carcinoma - Pathophysiology and ManagementDocument6 pagesBasal Cell Carcinoma - Pathophysiology and ManagementReylan Garcia0% (1)
- The Hypnosis Treatment Option: Proven Solutions For Pain, Insomnia, Stress, Obesity, and Other Common Health ProblemsDocument54 pagesThe Hypnosis Treatment Option: Proven Solutions For Pain, Insomnia, Stress, Obesity, and Other Common Health ProblemsCopper Ridge Press100% (5)
- K-45 Pharmacology of Uterotonics & TocolyticsDocument55 pagesK-45 Pharmacology of Uterotonics & TocolyticsJane Andrea Christiano Djianzonie100% (1)
- Persons Case Formulation ArticleDocument11 pagesPersons Case Formulation ArticleMarco Sousa100% (2)
- En GoutDocument2 pagesEn GoutJane Andrea Christiano DjianzoniePas encore d'évaluation
- Arrhythmia and Heart EmergenciesDocument57 pagesArrhythmia and Heart EmergenciesJane Andrea Christiano DjianzoniePas encore d'évaluation
- Bab 150 Hemopoesis PDFDocument3 pagesBab 150 Hemopoesis PDFJane Andrea Christiano DjianzoniePas encore d'évaluation
- English Test Guide and Structure GrammarDocument20 pagesEnglish Test Guide and Structure GrammarpLangpLingpLungPas encore d'évaluation
- K.7 & 8 Hormone Reproductive SystDocument55 pagesK.7 & 8 Hormone Reproductive SystsutansikandarPas encore d'évaluation
- K - 65 Farmakodinamik Dan Farmakokinetik Kontrasepsi TDocument24 pagesK - 65 Farmakodinamik Dan Farmakokinetik Kontrasepsi TJane Andrea Christiano DjianzoniePas encore d'évaluation
- Blok Reproductive System: Prof. Dr. Abdul Rasyid, Sprad, PHDDocument46 pagesBlok Reproductive System: Prof. Dr. Abdul Rasyid, Sprad, PHDJane Andrea Christiano DjianzoniePas encore d'évaluation
- En GoutDocument2 pagesEn GoutJane Andrea Christiano DjianzoniePas encore d'évaluation
- K 74-75 Pathology of UterusDocument51 pagesK 74-75 Pathology of UterusJane Andrea Christiano Djianzonie100% (1)
- Blok Reproductive System: Prof. Dr. Abdul Rasyid, Sprad, PHDDocument46 pagesBlok Reproductive System: Prof. Dr. Abdul Rasyid, Sprad, PHDJane Andrea Christiano DjianzoniePas encore d'évaluation
- (K11-K12) Fisiologi KehamilanDocument76 pages(K11-K12) Fisiologi KehamilanJane Andrea Christiano DjianzoniePas encore d'évaluation
- (k10) Ginecologic ExaminationDocument23 pages(k10) Ginecologic ExaminationJane Andrea Christiano DjianzoniePas encore d'évaluation
- (K5-K6) Hormon Repro Pria Dan Wanita, EditDocument53 pages(K5-K6) Hormon Repro Pria Dan Wanita, EditJane Andrea Christiano DjianzoniePas encore d'évaluation
- K - 12 Candidiasis (Mikrobiologi)Document38 pagesK - 12 Candidiasis (Mikrobiologi)Vedora Angelia GultomPas encore d'évaluation
- (k10) Ginecologic ExaminationDocument23 pages(k10) Ginecologic ExaminationJane Andrea Christiano DjianzoniePas encore d'évaluation
- K 7 - 9 Hormone Reproductive Syst.Document52 pagesK 7 - 9 Hormone Reproductive Syst.Jane Andrea Christiano DjianzoniePas encore d'évaluation
- (K2) Histo Female Reproductive System 2012Document81 pages(K2) Histo Female Reproductive System 2012Jane Andrea Christiano DjianzoniePas encore d'évaluation
- Neonatology Division Medical SchoolDocument22 pagesNeonatology Division Medical SchoolJane Andrea Christiano DjianzoniePas encore d'évaluation
- Complete Newborn Physical Exam ChecklistDocument44 pagesComplete Newborn Physical Exam ChecklistJosephine IrenaPas encore d'évaluation
- Physiology of Pregnancy Implantation and PlacentaDocument80 pagesPhysiology of Pregnancy Implantation and PlacentaJane Andrea Christiano DjianzoniePas encore d'évaluation
- K 5-6 Fungsi Hormone ReproduksiDocument54 pagesK 5-6 Fungsi Hormone ReproduksiJane Andrea Christiano DjianzoniePas encore d'évaluation
- Gestational Trophoblastic Neoplasia (KBK)Document22 pagesGestational Trophoblastic Neoplasia (KBK)Jane Andrea Christiano DjianzoniePas encore d'évaluation
- Ovarian Carsinoma (KBK)Document25 pagesOvarian Carsinoma (KBK)Jane Andrea Christiano DjianzoniePas encore d'évaluation
- k8 Biokim Hormon GdsDocument35 pagesk8 Biokim Hormon GdsRobert HallPas encore d'évaluation
- K.3b HORMONE CONTROL OF GROWTHDocument22 pagesK.3b HORMONE CONTROL OF GROWTHJane Andrea Christiano DjianzoniePas encore d'évaluation
- Coughlin CC Case Study IntroDocument3 pagesCoughlin CC Case Study Introapi-283315953100% (1)
- Tut 3Document3 pagesTut 3Bobet ReñaPas encore d'évaluation
- Perianal Problems: ACS/ASE Medical Student Core Curriculum Perianal ProblemsDocument21 pagesPerianal Problems: ACS/ASE Medical Student Core Curriculum Perianal ProblemsHasti Chande100% (1)
- Pertanyaan ReferatDocument2 pagesPertanyaan ReferatBuydh BfdsfsPas encore d'évaluation
- Typical, Atypical Optic NeuritisDocument10 pagesTypical, Atypical Optic NeuritisScerbatiuc CristinaPas encore d'évaluation
- CPG Diabetic NephropathyDocument23 pagesCPG Diabetic NephropathyapalaginihPas encore d'évaluation
- Persuasive - GR 11-27 AugustDocument1 pagePersuasive - GR 11-27 AugustShourya PanwarPas encore d'évaluation
- Oral and Maxillofacial Surgery Clinics of North America Office Based Anesthesia 45 57Document13 pagesOral and Maxillofacial Surgery Clinics of North America Office Based Anesthesia 45 57Max FaxPas encore d'évaluation
- Role of OT in Rett SyndromeDocument2 pagesRole of OT in Rett SyndromeDanielle Stella N'LucaPas encore d'évaluation
- Guideline On Anterior Cruciate Ligament Injury: A Multidisciplinary Review by The Dutch Orthopaedic AssociationDocument8 pagesGuideline On Anterior Cruciate Ligament Injury: A Multidisciplinary Review by The Dutch Orthopaedic Associationbagus arisPas encore d'évaluation
- 2 2 15 923 PDFDocument4 pages2 2 15 923 PDFwatidina100% (1)
- Willard 2007 GastroenterologíaDocument65 pagesWillard 2007 GastroenterologíaHazel.Pas encore d'évaluation
- RSBY Hospital Manual 28072010Document44 pagesRSBY Hospital Manual 28072010chimera03Pas encore d'évaluation
- Rabbit FeedDocument2 pagesRabbit FeedDaniel T. AdamaPas encore d'évaluation
- Gerontology Case Study: Age-Related RisksDocument14 pagesGerontology Case Study: Age-Related RisksAna BiennePas encore d'évaluation
- Scenicview Academy-1Document54 pagesScenicview Academy-1api-380681224Pas encore d'évaluation
- Orig 1 S 000 Other RDocument37 pagesOrig 1 S 000 Other RCastle SkyPas encore d'évaluation
- PHRM TemplateDocument4 pagesPHRM TemplateRichard SakyiamahPas encore d'évaluation
- ATT Induced Hepatotoxicity: Dr. K. K. SharmaDocument36 pagesATT Induced Hepatotoxicity: Dr. K. K. SharmaSucharita Ray100% (1)
- Jazzle George E. Oteyza NCMB 312 Rle BSN 3Y1-3A Lab Module Course TaskDocument3 pagesJazzle George E. Oteyza NCMB 312 Rle BSN 3Y1-3A Lab Module Course TaskwokorowPas encore d'évaluation
- MinimizingDocument5 pagesMinimizingAryananda Kondre AndikaPas encore d'évaluation
- World Health OrganizationDocument27 pagesWorld Health OrganizationrhazamPas encore d'évaluation
- Pricelis HargaDocument30 pagesPricelis Hargadwi mulyaningsihPas encore d'évaluation
- Postgraduate Certificate in Clinical Psychology - Level 7Document4 pagesPostgraduate Certificate in Clinical Psychology - Level 7Revathy KrishnaPas encore d'évaluation