Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Pathophysiology of PreeclampsiaDocument1 pagePathophysiology of PreeclampsiaKristine Alejandro100% (14)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Prehospital Emergency Care 11th Edition 11th EditionDocument61 pagesPrehospital Emergency Care 11th Edition 11th Editionmarion.wade94398% (42)
- Coronary Artery Disease Pathophysiology PDFDocument3 pagesCoronary Artery Disease Pathophysiology PDFMohd Amir Bin Bashir0% (1)
- UWorld Step 2 CK Notes - 2015Document4 pagesUWorld Step 2 CK Notes - 2015Ernesto Prado67% (3)
- IWGDF Guidelines On The Prevention and Management of Diabetic Foot Disease 2019Document47 pagesIWGDF Guidelines On The Prevention and Management of Diabetic Foot Disease 2019Sidan EmoziePas encore d'évaluation
- Role of Vacuum Assisted Closure (VAC) in Treatment of Difficult To Heal Wounds in Lower Extremity - Our Experience in 100 CasesDocument8 pagesRole of Vacuum Assisted Closure (VAC) in Treatment of Difficult To Heal Wounds in Lower Extremity - Our Experience in 100 CasesSidan EmoziePas encore d'évaluation
- Spontaneous Pneumothorax As Unusual Presenting Symptom of COVID-19 Pneumonia: Surgical Management and Pathological FindingsDocument5 pagesSpontaneous Pneumothorax As Unusual Presenting Symptom of COVID-19 Pneumonia: Surgical Management and Pathological FindingsSidan EmoziePas encore d'évaluation
- Diabetic Foot and Foot Debridement TechniqueDocument14 pagesDiabetic Foot and Foot Debridement TechniqueSidan EmoziePas encore d'évaluation
- Research: The Profile of Patients With Obstructive Uropathy in Cameroon: Case of The Douala General HospitalDocument6 pagesResearch: The Profile of Patients With Obstructive Uropathy in Cameroon: Case of The Douala General HospitalSidan EmoziePas encore d'évaluation
- Diabetic Foot and Foot Debridement Technique: Wound ManagementDocument5 pagesDiabetic Foot and Foot Debridement Technique: Wound ManagementAlex Gino Quispe EnriquezPas encore d'évaluation
- Upper Extremity FracturesDocument80 pagesUpper Extremity FracturesSidan EmoziePas encore d'évaluation
- Tseng2009 PDFDocument7 pagesTseng2009 PDFArthana PutraPas encore d'évaluation
- Identification of Common Orthopaedic CasesDocument4 pagesIdentification of Common Orthopaedic CasesSidan EmoziePas encore d'évaluation
- Upper Extremity FracturesDocument80 pagesUpper Extremity FracturesSidan EmoziePas encore d'évaluation
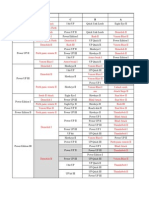
- Table Skill Pet Heva ADocument32 pagesTable Skill Pet Heva ASidan EmoziePas encore d'évaluation
- Hepatopulmonary Syndrome (HPS) : by Alaa Haseeb, MS.CDocument27 pagesHepatopulmonary Syndrome (HPS) : by Alaa Haseeb, MS.CSidan EmoziePas encore d'évaluation
- Assessment Nursing Diagnosis Scientific Explanation Planning Nursing Intervention RationaleDocument3 pagesAssessment Nursing Diagnosis Scientific Explanation Planning Nursing Intervention Rationalekimglaidyl bontuyanPas encore d'évaluation
- FEU Review Pre Board Exam 2016 PathophysioDocument8 pagesFEU Review Pre Board Exam 2016 PathophysioDharlyn MungcalPas encore d'évaluation
- CASEDocument9 pagesCASELeah SorianoPas encore d'évaluation
- First Summative Test in Science 9Document2 pagesFirst Summative Test in Science 9Anna Mae A. Pamonag100% (1)
- 13.1 HomeostasisDocument9 pages13.1 HomeostasistemkemPas encore d'évaluation
- Acute PainDocument1 pageAcute PainJohn Herrera TanchuanPas encore d'évaluation
- News DilaDocument1 pageNews DilaferraPas encore d'évaluation
- Activity 2 Cardiac Drug StudyDocument5 pagesActivity 2 Cardiac Drug StudyKlai ArriolaPas encore d'évaluation
- Immediate Physiological Changes in New BornDocument7 pagesImmediate Physiological Changes in New BornLahunWanniangPas encore d'évaluation
- Mwenge Catholic University (Mwecau) Departiment of Natural Science and Information TechnologyDocument3 pagesMwenge Catholic University (Mwecau) Departiment of Natural Science and Information TechnologyPaulo DanielPas encore d'évaluation
- Chapter 2 - Examination of Vital SignsDocument85 pagesChapter 2 - Examination of Vital SignsAudrrey LewisPas encore d'évaluation
- 4 PharmacodynamicsDocument21 pages4 Pharmacodynamicsaimi BatrisyiaPas encore d'évaluation
- Heart Failure Lily ModifiedDocument57 pagesHeart Failure Lily ModifiedSabila FatimahPas encore d'évaluation
- Gap Co2 Cocc 2018Document9 pagesGap Co2 Cocc 2018Cesar Rivas CamposPas encore d'évaluation
- Cardiac Inspection and Palpation CardiologyDocument25 pagesCardiac Inspection and Palpation CardiologyMohamed El SayedPas encore d'évaluation
- Nervous System WSHDocument2 pagesNervous System WSHArdra AnilPas encore d'évaluation
- FLG 332 Renal Physiology - 1 (2019)Document58 pagesFLG 332 Renal Physiology - 1 (2019)Huzaifa KhanPas encore d'évaluation
- Ob NCP 2Document2 pagesOb NCP 2Kimberly Mondala (SHS)Pas encore d'évaluation
- Overview - HUMAN BLOOD CIRCULATION AND PATHWAYSDocument2 pagesOverview - HUMAN BLOOD CIRCULATION AND PATHWAYSDj22 JakePas encore d'évaluation
- General Biology 1 (SHS) : The Two Shades of GreenDocument18 pagesGeneral Biology 1 (SHS) : The Two Shades of GreenLAN soajasPas encore d'évaluation
- CHAPTER 10 - CONTROL OF BODY MOVEMENT (Akdemics)Document6 pagesCHAPTER 10 - CONTROL OF BODY MOVEMENT (Akdemics)Ivy CustodioPas encore d'évaluation
- Key of SEQs Heart, Nerve and Muscle Revision TestDocument11 pagesKey of SEQs Heart, Nerve and Muscle Revision TestMudassar Roomi100% (2)
- KS3 Human Organ SystemDocument2 pagesKS3 Human Organ Systemejljn1Pas encore d'évaluation
- CVS ElectrocardiogramDocument167 pagesCVS ElectrocardiogramSheral AidaPas encore d'évaluation
- Penetrating Abdominal Trauma (Stab Wound)Document1 pagePenetrating Abdominal Trauma (Stab Wound)P BPas encore d'évaluation