Vous aimerez peut-être aussi
- Pulmonary TuberculosisDocument38 pagesPulmonary TuberculosisHiba AssiPas encore d'évaluation
- AN AIDS PATIENT WITH CRYPTOCOCCUS NEOFORMANS PNEUMONIADocument26 pagesAN AIDS PATIENT WITH CRYPTOCOCCUS NEOFORMANS PNEUMONIABrinna Anindita SatriaPas encore d'évaluation
- Clinical Practice Guideline On Diagnosis and Treatment of Hyponatremia PDFDocument12 pagesClinical Practice Guideline On Diagnosis and Treatment of Hyponatremia PDFLuis Mochas HClPas encore d'évaluation
- Anaphylaxis GuideDocument27 pagesAnaphylaxis Guidenadya idfentiPas encore d'évaluation
- Jambore-Pkb (Lazuardi Dwipa, DR - SPPD, K-Ger)Document65 pagesJambore-Pkb (Lazuardi Dwipa, DR - SPPD, K-Ger)UPT PKM UJUNGBERUNG INDAHPas encore d'évaluation
- Spektrum AIDocument55 pagesSpektrum AIOgizWaraPas encore d'évaluation
- Metabolic Disorders in Emergency OncologyDocument27 pagesMetabolic Disorders in Emergency Oncologytepat rshsPas encore d'évaluation
- TK - Peran CA 125Document25 pagesTK - Peran CA 125Farli Wenang MaradjabessyPas encore d'évaluation
- SEO-Optimized Title for PBC Case ReportDocument40 pagesSEO-Optimized Title for PBC Case Reportv_vijayakanth7656Pas encore d'évaluation
- S1.1 Ria Bandiara - Role Managemen Hypertension PKB 2019Document29 pagesS1.1 Ria Bandiara - Role Managemen Hypertension PKB 2019siputleletPas encore d'évaluation
- WS 5 - DR DR C Heriawan Soejono, SPPD, KGer, M.Epid, MPH - TATALAKSANA PASIEN GERIATRI PDFDocument34 pagesWS 5 - DR DR C Heriawan Soejono, SPPD, KGer, M.Epid, MPH - TATALAKSANA PASIEN GERIATRI PDFApres SyahwaPas encore d'évaluation
- DR Aida Lombok 3 Mei 2017 - HisfarsiDocument39 pagesDR Aida Lombok 3 Mei 2017 - HisfarsiBasri BaslamPas encore d'évaluation
- Manage Anemia in CKD Patients: Iron Therapy GuidelinesDocument36 pagesManage Anemia in CKD Patients: Iron Therapy GuidelinesLaurensia Erlina NataliaPas encore d'évaluation
- 1 Cardiorenal SyndromeDocument71 pages1 Cardiorenal SyndromeHermann HernandezPas encore d'évaluation
- CKDMMM 150717231019 Lva1 App6892 PDFDocument47 pagesCKDMMM 150717231019 Lva1 App6892 PDFTabada NickyPas encore d'évaluation
- Detection of Brucella Species in ApparentlyDocument21 pagesDetection of Brucella Species in ApparentlyHubdar Ali KolachiPas encore d'évaluation
- Brucellosis: Aka: Mediterranean Fever, Malta Fever, Gastric Remittent Fever, and Undulant FeverDocument11 pagesBrucellosis: Aka: Mediterranean Fever, Malta Fever, Gastric Remittent Fever, and Undulant Feverfairuz160194Pas encore d'évaluation
- Prof. Syakib Acute Kidney Injury - Internal Medicine Emergency Course - Agustus 2019-DikonversiDocument35 pagesProf. Syakib Acute Kidney Injury - Internal Medicine Emergency Course - Agustus 2019-DikonversidrroytambunanPas encore d'évaluation
- BCCA Febrile Neutropenia GuidelinesDocument2 pagesBCCA Febrile Neutropenia GuidelinesdenokayuMRPas encore d'évaluation
- Hepatitis BDocument22 pagesHepatitis BLina VmalePas encore d'évaluation
- Modul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaDocument22 pagesModul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaYhaya 'Dzulhijjahyanti'Pas encore d'évaluation
- GLomerulus DiseaseDocument5 pagesGLomerulus DiseaseMEDS easyPas encore d'évaluation
- Brucellosis DeseaseDocument18 pagesBrucellosis DeseaseDwiki RamadhanPas encore d'évaluation
- Emerging Infection Disease Vol 24 No 8 Tahun 2018Document216 pagesEmerging Infection Disease Vol 24 No 8 Tahun 2018anyPas encore d'évaluation
- 04 Hemoglobin HemoglobinopathiesDocument32 pages04 Hemoglobin HemoglobinopathiesBianca OcampoPas encore d'évaluation
- Systematic Approach in Anemia Evaluation and Review of Peripheral SmearsDocument72 pagesSystematic Approach in Anemia Evaluation and Review of Peripheral SmearsSukma Eka PratiwiPas encore d'évaluation
- Doac Vs LMWHDocument6 pagesDoac Vs LMWHTry Enos OktafianPas encore d'évaluation
- Venous Thromboemboly in Covid-19: DR. Dr. Idar Mappangara, SP - PD, SP - JP (K)Document30 pagesVenous Thromboemboly in Covid-19: DR. Dr. Idar Mappangara, SP - PD, SP - JP (K)haeriah sabaruddinPas encore d'évaluation
- Lung CancerDocument33 pagesLung CancerPirma Ivan Ricky MPas encore d'évaluation
- Hemoglobin Electrophoresis EditedDocument48 pagesHemoglobin Electrophoresis EditedBean TePas encore d'évaluation
- Disseminated Intravacular Coagulation (DIC) 2Document12 pagesDisseminated Intravacular Coagulation (DIC) 2Radya AgnaPas encore d'évaluation
- GlomerulonephritisDocument59 pagesGlomerulonephritistressPas encore d'évaluation
- Bimbingan Dokter Hari - CKDDocument24 pagesBimbingan Dokter Hari - CKDVicky LumalessilPas encore d'évaluation
- Apheresis: (Principle & Clinical Applications)Document35 pagesApheresis: (Principle & Clinical Applications)aprinalPas encore d'évaluation
- Hiv-Associated Nephropathy (Hivan) : DR KibaruDocument27 pagesHiv-Associated Nephropathy (Hivan) : DR KibaruMalueth AnguiPas encore d'évaluation
- Role of BNP and NT-proBNP in diagnosing heart failureDocument7 pagesRole of BNP and NT-proBNP in diagnosing heart failureyehezkieldwardPas encore d'évaluation
- Chronic Liver DiseaseDocument3 pagesChronic Liver DiseaseMohammad AbbasPas encore d'évaluation
- Sepsis and Septic Shock GuidelinesfinalDocument51 pagesSepsis and Septic Shock GuidelinesfinalElteyb Nor eldaimPas encore d'évaluation
- Name: Ra Tuty Kuswardhani Md. PHD, Mha, Finasim, Geriatrician Pembina Utama Madya / Iv D/ Head LectorDocument27 pagesName: Ra Tuty Kuswardhani Md. PHD, Mha, Finasim, Geriatrician Pembina Utama Madya / Iv D/ Head LectorMardikaPas encore d'évaluation
- Integrated Therapeutics-Ii For 3 Year STS: Chapter-1Document69 pagesIntegrated Therapeutics-Ii For 3 Year STS: Chapter-1Geleta GalataaPas encore d'évaluation
- Zoonotic Bacteria: BrucellaDocument13 pagesZoonotic Bacteria: BrucellaNagender UpadhyayPas encore d'évaluation
- Kul Sem 4 Heat Stroke N Fever UHT 2016Document63 pagesKul Sem 4 Heat Stroke N Fever UHT 2016NandaSuryaWijayaPas encore d'évaluation
- CholestasisDocument39 pagesCholestasisMukhtar JamacPas encore d'évaluation
- 2.abdominal TuberculosisDocument8 pages2.abdominal Tuberculosisram krishnaPas encore d'évaluation
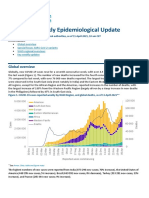
- COVID-19 Weekly Epidemiological Update: Global OverviewDocument31 pagesCOVID-19 Weekly Epidemiological Update: Global OverviewPaolaPas encore d'évaluation
- Ami Ashariati - Immunotherapy in CancerDocument142 pagesAmi Ashariati - Immunotherapy in CancersarijuicyPas encore d'évaluation
- Pancreatic MalignancyDocument22 pagesPancreatic Malignancylovelots1234Pas encore d'évaluation
- Penyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUDocument56 pagesPenyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUFitriana WijayatiPas encore d'évaluation
- Sindrom KardiorenalDocument12 pagesSindrom KardiorenalAndreAHutasoitPas encore d'évaluation
- Myeloproliferative Disorders 18th Oct 2010Document62 pagesMyeloproliferative Disorders 18th Oct 2010saint5470Pas encore d'évaluation
- Tubulointerstitial Diseases: Dr. Raid JastaniaDocument48 pagesTubulointerstitial Diseases: Dr. Raid JastaniaThomas McconnellPas encore d'évaluation
- Natriuretic Peptide System DiagnosisDocument30 pagesNatriuretic Peptide System DiagnosisKhaled S. HarbPas encore d'évaluation
- HCV diagnostic and health care worker managementDocument36 pagesHCV diagnostic and health care worker managementLaboratorium Ansari SalehPas encore d'évaluation
- Emergency Medicine-Aru W. SudoyoDocument44 pagesEmergency Medicine-Aru W. SudoyoArdhiPas encore d'évaluation
- REFERAT DMARDsDocument42 pagesREFERAT DMARDsBhayu Dharma SuryanaPas encore d'évaluation
- Diagnosis and Management of Upper Gastrointestinal Bleeding PDFDocument10 pagesDiagnosis and Management of Upper Gastrointestinal Bleeding PDFKetut Suwadiaya P AdnyanaPas encore d'évaluation
- Hepatitis B Serodiagnosis EssentialsDocument4 pagesHepatitis B Serodiagnosis EssentialsMarc Imhotep Cray, M.D.Pas encore d'évaluation
- PansitopeniaDocument33 pagesPansitopeniaBrad WrightPas encore d'évaluation
- Pemeriksaan Terkini Hepatitis Virus: Prof. Dr. Jusak Nugraha, DR, MS, SPPK (K) Lab Patologi Klinik FK UnairDocument53 pagesPemeriksaan Terkini Hepatitis Virus: Prof. Dr. Jusak Nugraha, DR, MS, SPPK (K) Lab Patologi Klinik FK UnairMuh YunusPas encore d'évaluation
- Kuliah YyDocument26 pagesKuliah YyEsakumala DinantiPas encore d'évaluation
- Reiner2017 PDFDocument8 pagesReiner2017 PDFjessicaPas encore d'évaluation
- Blakytny 2009Document11 pagesBlakytny 2009jessicaPas encore d'évaluation
- 10 1001@jama 2017 11700Document2 pages10 1001@jama 2017 11700jessicaPas encore d'évaluation
- NT Sep13Document20 pagesNT Sep13jessicaPas encore d'évaluation
- Reiner2017 PDFDocument8 pagesReiner2017 PDFjessicaPas encore d'évaluation
- Ibnt 06 I 2 P 229Document4 pagesIbnt 06 I 2 P 229jessicaPas encore d'évaluation
- 1730 6013 3 PBDocument4 pages1730 6013 3 PBjessicaPas encore d'évaluation
- Rattan 2008Document6 pagesRattan 2008jessicaPas encore d'évaluation
- Diabetic Foot Infection: Antibiotic Therapy and Good Practice RecommendationsDocument10 pagesDiabetic Foot Infection: Antibiotic Therapy and Good Practice RecommendationsjessicaPas encore d'évaluation
- Glaude Mans 2015Document43 pagesGlaude Mans 2015jessicaPas encore d'évaluation
- Proliferation Inhibition and Apoptosis Induction of Imatinib-Resistant Chronic Myeloid Leukemia Cells Via PPP2R5C Down-RegulationDocument12 pagesProliferation Inhibition and Apoptosis Induction of Imatinib-Resistant Chronic Myeloid Leukemia Cells Via PPP2R5C Down-RegulationjessicaPas encore d'évaluation
- Innovation in Healthcare Delivery Systems FrameworkDocument20 pagesInnovation in Healthcare Delivery Systems FrameworkRirin NurmandhaniPas encore d'évaluation
- 6 Step Problem SolvingDocument9 pages6 Step Problem SolvingjessicaPas encore d'évaluation
- Guideline MpsDocument15 pagesGuideline MpsjessicaPas encore d'évaluation
- Getachew4352013BJMMR7308 1Document10 pagesGetachew4352013BJMMR7308 1jessicaPas encore d'évaluation
- Comparing Radiological Features of Pulmonary Tuberculosis With and Without Hiv Infection 2155 6113.1000188Document3 pagesComparing Radiological Features of Pulmonary Tuberculosis With and Without Hiv Infection 2155 6113.1000188Riot Riot AdjaPas encore d'évaluation
- 50 Supplement - 3 S223 PDFDocument8 pages50 Supplement - 3 S223 PDFjessicaPas encore d'évaluation
- TB and HIV - Co-Infection, Diagnosis & TreatmentDocument5 pagesTB and HIV - Co-Infection, Diagnosis & TreatmentjessicaPas encore d'évaluation
- How To Write An Academic JournalDocument113 pagesHow To Write An Academic JournaljessicaPas encore d'évaluation
- Clinical Mentoring 10 Kegawatan Jantung Oleh Dr. Ika Prasetya Wijayasppd KKV Finasim FacpDocument48 pagesClinical Mentoring 10 Kegawatan Jantung Oleh Dr. Ika Prasetya Wijayasppd KKV Finasim FacpGede GiriPas encore d'évaluation
- Clinical and Radiographic Manifestations and Treatment Outcome of Pulmonary Tuberculosis in The Elderly in Khuzestan, Southwest IranDocument6 pagesClinical and Radiographic Manifestations and Treatment Outcome of Pulmonary Tuberculosis in The Elderly in Khuzestan, Southwest IranjessicaPas encore d'évaluation
- Alkindi 2016Document3 pagesAlkindi 2016jessicaPas encore d'évaluation
- Ifnγ-Producing Cd4 T Lymphocytes: The Double-Edged Swords In TuberculosisDocument7 pagesIfnγ-Producing Cd4 T Lymphocytes: The Double-Edged Swords In TuberculosisjessicaPas encore d'évaluation
- 1 s2.0 S0422763816300796 Main PDFDocument9 pages1 s2.0 S0422763816300796 Main PDFjessicaPas encore d'évaluation
- Epidemiology of Tuberculosis and HIV Coinfections in Singapore, 2000 2014Document6 pagesEpidemiology of Tuberculosis and HIV Coinfections in Singapore, 2000 2014jessicaPas encore d'évaluation
- Microscopy As A Diagnostic Tool in Pulmonary Tuberculosis: SciencedirectDocument6 pagesMicroscopy As A Diagnostic Tool in Pulmonary Tuberculosis: SciencedirectjessicaPas encore d'évaluation
- 1 s2.0 S0196064410013223 MainDocument14 pages1 s2.0 S0196064410013223 MainjessicaPas encore d'évaluation
- Epidemiology of Tuberculosis and HIV Coinfections in Singapore, 2000 2014Document6 pagesEpidemiology of Tuberculosis and HIV Coinfections in Singapore, 2000 2014jessicaPas encore d'évaluation
- Role of CultureDocument6 pagesRole of CulturejessicaPas encore d'évaluation
- Comparative Ethnographies: State and Its MarginsDocument31 pagesComparative Ethnographies: State and Its MarginsJuan ManuelPas encore d'évaluation
- Liquid Hydrogen As A Propulsion Fuel, 1945-1959Document341 pagesLiquid Hydrogen As A Propulsion Fuel, 1945-1959Bob AndrepontPas encore d'évaluation
- PRINCE2 Product Map Timeline Diagram (v1.5)Document11 pagesPRINCE2 Product Map Timeline Diagram (v1.5)oblonggroupPas encore d'évaluation
- Mr. Honey's Large Business DictionaryEnglish-German by Honig, WinfriedDocument538 pagesMr. Honey's Large Business DictionaryEnglish-German by Honig, WinfriedGutenberg.orgPas encore d'évaluation
- Causes and Diagnosis of Iron Deficiency and Iron Deficiency Anemia in AdultsDocument88 pagesCauses and Diagnosis of Iron Deficiency and Iron Deficiency Anemia in AdultsGissell LópezPas encore d'évaluation
- Speakout Vocabulary Extra Advanced Unit 03Document3 pagesSpeakout Vocabulary Extra Advanced Unit 03shasha1982100% (2)
- Think Like An EconomistDocument34 pagesThink Like An EconomistDiv-yuh BothraPas encore d'évaluation
- GII-07 Training MaterialDocument191 pagesGII-07 Training MaterialIris Amati MartinsPas encore d'évaluation
- Combined RubricsDocument3 pagesCombined Rubricsapi-446053878Pas encore d'évaluation
- Chapter 9 MafinDocument36 pagesChapter 9 MafinReymilyn SanchezPas encore d'évaluation
- Henderson - Historical Documents of The Middle AgesDocument536 pagesHenderson - Historical Documents of The Middle AgesVlad VieriuPas encore d'évaluation
- Functional Appliances 2018Document45 pagesFunctional Appliances 2018tonhanrhmPas encore d'évaluation
- Sri Dakshinamurthy Stotram - Hindupedia, The Hindu EncyclopediaDocument7 pagesSri Dakshinamurthy Stotram - Hindupedia, The Hindu Encyclopediamachnik1486624Pas encore d'évaluation
- Raman Spectroscopy: 1 Theoretical BasisDocument9 pagesRaman Spectroscopy: 1 Theoretical BasisJèManziPas encore d'évaluation
- Why Research Is Important in The BusinessDocument2 pagesWhy Research Is Important in The BusinessBricx BalerosPas encore d'évaluation
- Foundation of Special and Inclusive EducationDocument25 pagesFoundation of Special and Inclusive Educationmarjory empredoPas encore d'évaluation
- Life Convict Laxman Naskar Vs State of West Bengal & Anr On 1 September, 2000Document6 pagesLife Convict Laxman Naskar Vs State of West Bengal & Anr On 1 September, 2000Kimberly HardyPas encore d'évaluation
- St. Louis ChemicalDocument8 pagesSt. Louis ChemicalNaomi Alberg-BlijdPas encore d'évaluation
- INTERNSHIP REPORT 3 PagesDocument4 pagesINTERNSHIP REPORT 3 Pagesali333444Pas encore d'évaluation
- Viennas Cafe Louvre in The 1920s and 1930Document18 pagesViennas Cafe Louvre in The 1920s and 1930Friso HoeneveldPas encore d'évaluation
- APCHG 2019 ProceedingsDocument69 pagesAPCHG 2019 ProceedingsEnrico SocoPas encore d'évaluation
- The Forty Nine StepsDocument312 pagesThe Forty Nine Stepsoldnic67% (3)
- Ad844 PDFDocument20 pagesAd844 PDFkavi_mishra92Pas encore d'évaluation
- School For Good and EvilDocument4 pagesSchool For Good and EvilHaizyn RizoPas encore d'évaluation
- Parashara'S Light 7.0.1 (C) Geovision Software, Inc., Licensed ToDocument5 pagesParashara'S Light 7.0.1 (C) Geovision Software, Inc., Licensed TobrajwasiPas encore d'évaluation
- Table Topics Contest Toastmaster ScriptDocument4 pagesTable Topics Contest Toastmaster ScriptchloephuahPas encore d'évaluation
- Chapter 10 HandoutDocument18 pagesChapter 10 HandoutChad FerninPas encore d'évaluation
- Merry Almost Christmas - A Year With Frog and Toad (Harmonies)Document6 pagesMerry Almost Christmas - A Year With Frog and Toad (Harmonies)gmit92Pas encore d'évaluation
- The Islam Question - Should I Become A Muslim?Document189 pagesThe Islam Question - Should I Become A Muslim?Aorounga100% (1)