Vous aimerez peut-être aussi
- Curing Stage 4 Cancer and Terminal Liver Disease with Alpha Lipoic AcidDocument14 pagesCuring Stage 4 Cancer and Terminal Liver Disease with Alpha Lipoic Acidguy777Pas encore d'évaluation
- Antibody Screening and IDDocument60 pagesAntibody Screening and IDPamela MendozaPas encore d'évaluation
- Boolean AlgebraDocument29 pagesBoolean AlgebraDeepanshuPas encore d'évaluation
- Lester Desjarlais Inquest Parts I and IIDocument108 pagesLester Desjarlais Inquest Parts I and IIJames Turner100% (1)
- Comprehensive Schools Safety Monitoring ChecklistDocument5 pagesComprehensive Schools Safety Monitoring ChecklistKriss Paran100% (1)
- Sampling Methods GuideDocument35 pagesSampling Methods GuideKim RamosPas encore d'évaluation
- Computer Servicing 4: Introduction To Logic Gates Boolean AlgebraDocument13 pagesComputer Servicing 4: Introduction To Logic Gates Boolean AlgebraJhon Keneth NamiasPas encore d'évaluation
- Obstetrics and Gynecology Question PapersDocument22 pagesObstetrics and Gynecology Question Papersprinceej83% (18)
- TIVA Part I - Pharmacokinetic Principles and Methods of Delivery PDFDocument56 pagesTIVA Part I - Pharmacokinetic Principles and Methods of Delivery PDFMaria José RechePas encore d'évaluation
- Antibody PanelDocument81 pagesAntibody PanelMa. Pe Delaine MendrosPas encore d'évaluation
- Ab Screening PDFDocument67 pagesAb Screening PDFJerome ValerianoPas encore d'évaluation
- DR - Usi-Screening & Identification AntibodyDocument44 pagesDR - Usi-Screening & Identification AntibodySukma EffendyPas encore d'évaluation
- Pre Transfusion TestingDocument67 pagesPre Transfusion TestingPaulino GarciaPas encore d'évaluation
- Detection and Identification of Antibodies - SCDocument67 pagesDetection and Identification of Antibodies - SCLyra Dennise LlidoPas encore d'évaluation
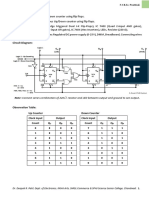
- SY - Synchronous Counter Using Flip FlopsDocument2 pagesSY - Synchronous Counter Using Flip FlopsAbhishek ParmarPas encore d'évaluation
- BMA Lab Report Digital IIDocument7 pagesBMA Lab Report Digital IIAmine usmaPas encore d'évaluation
- 2 Raos ISBT Immunohematology WP Case Study 1 FINAL PDFDocument31 pages2 Raos ISBT Immunohematology WP Case Study 1 FINAL PDFdrtsotlhe mogolegwaPas encore d'évaluation
- Chapter #5: Programmable Logic ControllerDocument30 pagesChapter #5: Programmable Logic ControllerPavi TranPas encore d'évaluation
- Advanced Immunohematology TechniquesDocument47 pagesAdvanced Immunohematology TechniquesPamela MendozaPas encore d'évaluation
- Demp Session - 2 VPDocument65 pagesDemp Session - 2 VPRAHUL KUMAR RPas encore d'évaluation
- Assignment 1 DSE 163Document4 pagesAssignment 1 DSE 163sandunmaheesha01Pas encore d'évaluation
- Ex No:4 Code Convertors: CS2207-Digital LabDocument7 pagesEx No:4 Code Convertors: CS2207-Digital LabSuresh Babu PalpandiPas encore d'évaluation
- Format Pelaporan Logistik NonARV 2022 - Rev LAYANAN MEDANDocument6 pagesFormat Pelaporan Logistik NonARV 2022 - Rev LAYANAN MEDANJava GreenPas encore d'évaluation
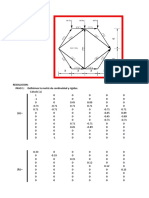
- Problem Table Algorithm: Company NameDocument1 pageProblem Table Algorithm: Company NameGiussepi Ali Jhonatan Mamani PacoPas encore d'évaluation
- CELEBROWDocument16 pagesCELEBROWEpaja Jeremiah JessePas encore d'évaluation
- Problem Table Algorithm: Company NameDocument1 pageProblem Table Algorithm: Company NameGloria Elena PerezPas encore d'évaluation
- Laporan Bulanan Rekapitulasi Surveilans Terpadu Penyakit (STP) Baru Di Puskesmas Dan Jejaringnya Puskesmas SoliuDocument37 pagesLaporan Bulanan Rekapitulasi Surveilans Terpadu Penyakit (STP) Baru Di Puskesmas Dan Jejaringnya Puskesmas SoliuVictoria YanersPas encore d'évaluation
- Biodiversity Questions Vs Schemes (Totals (Others Hidden) )Document5 pagesBiodiversity Questions Vs Schemes (Totals (Others Hidden) )Matias JaraPas encore d'évaluation
- Hcin620 m6 Lab6 Hanifahmutesi-FinalprojectDocument5 pagesHcin620 m6 Lab6 Hanifahmutesi-Finalprojectapi-488096711Pas encore d'évaluation
- Tutorial 2 - Electronics (2018)Document3 pagesTutorial 2 - Electronics (2018)Pasindu PramodPas encore d'évaluation
- SURVEILANS PENYAKIT POSKESDES SUNGAI NIPAHDocument6 pagesSURVEILANS PENYAKIT POSKESDES SUNGAI NIPAHKiki febrianiPas encore d'évaluation
- LeeBL Lab 3 (Week 4)Document5 pagesLeeBL Lab 3 (Week 4)marksman471Pas encore d'évaluation
- Experiment No 18Document4 pagesExperiment No 18NEAYZ AHMADPas encore d'évaluation
- 3-bit asynchronous Up/Down counter flip-flopsDocument2 pages3-bit asynchronous Up/Down counter flip-flopsIshtiaque Ahmed TanimPas encore d'évaluation
- SURVEILANS PUSKESMAS SINGKAWANG BARAT IIDocument19 pagesSURVEILANS PUSKESMAS SINGKAWANG BARAT IIVelikaPas encore d'évaluation
- Capter 5Document53 pagesCapter 5surafel5248Pas encore d'évaluation
- Grade83rdQuarterSummativeTest-2024-03-24T13_14_57_462041-46399cDocument12 pagesGrade83rdQuarterSummativeTest-2024-03-24T13_14_57_462041-46399clabiosjasminPas encore d'évaluation
- VERIFICATIONDocument7 pagesVERIFICATIONNOV DAVANNPas encore d'évaluation
- 2019-01-23 - HiPEAC Tutorial - AritraDocument30 pages2019-01-23 - HiPEAC Tutorial - AritraAritra SarkarPas encore d'évaluation
- Survailans Terpadu Penyakit Berbasis Puskesmas (Kasus Baru) Per Golongan UmurDocument11 pagesSurvailans Terpadu Penyakit Berbasis Puskesmas (Kasus Baru) Per Golongan UmurtimgerakcepatpasmingPas encore d'évaluation
- Malaria 19 NewDocument106 pagesMalaria 19 NewmeckhyseranPas encore d'évaluation
- Combinational Logic Circuits Experiment 4Document11 pagesCombinational Logic Circuits Experiment 4Vince abcdPas encore d'évaluation
- E91 IntroDocument25 pagesE91 IntroAlekso GjakovskiPas encore d'évaluation
- 320 Into Binary:: Introduction To Computing (CS101)Document3 pages320 Into Binary:: Introduction To Computing (CS101)Hohaho YohahaPas encore d'évaluation
- Monthly Sanitation Clinic ReportDocument2 pagesMonthly Sanitation Clinic ReportForcus PuannPas encore d'évaluation
- Laporan Pws Penyakit 16032022surveilancefeb22Document4 pagesLaporan Pws Penyakit 16032022surveilancefeb22Covid petamburanPas encore d'évaluation
- Solución de problemas de estructuras 1Document12 pagesSolución de problemas de estructuras 1Jose Jean Ramos SerranoPas encore d'évaluation
- Digital AdesDocument17 pagesDigital AdesPraveen KishanPas encore d'évaluation
- Kelurahan: Pengadegan Wilayah:: Survailans Terpadu Penyakit (Kasus Baru) Per Golongan UmurDocument9 pagesKelurahan: Pengadegan Wilayah:: Survailans Terpadu Penyakit (Kasus Baru) Per Golongan UmurseptyPas encore d'évaluation
- 7 segDocument4 pages7 segPriti DheknePas encore d'évaluation
- Cse1003 DLD LabDocument14 pagesCse1003 DLD LabPranav Chaurasia 18BCE0216Pas encore d'évaluation
- Assement 04Document5 pagesAssement 04Naina PrasharPas encore d'évaluation
- Lab ReportDocument7 pagesLab Reportlesh allanoPas encore d'évaluation
- Akekaduro24_ 1894422Document15 pagesAkekaduro24_ 1894422Kelvin OppongPas encore d'évaluation
- Laporan LB 1 Februari 2021Document8 pagesLaporan LB 1 Februari 2021tugasPas encore d'évaluation
- PCB Reprt (1) FinalDocument8 pagesPCB Reprt (1) FinalShamma SPas encore d'évaluation
- SR .No. Name of Sheet StatusDocument6 pagesSR .No. Name of Sheet StatusMaheswaraRaoPas encore d'évaluation
- NOT/INVERTER Gate Lab ExerciseDocument5 pagesNOT/INVERTER Gate Lab ExerciseRicardo Edrell RiveraPas encore d'évaluation
- MalariaDocument130 pagesMalariainamulyatiumbunayPas encore d'évaluation
- Binary Addition and SubtractionDocument3 pagesBinary Addition and SubtractionRiaz KhanPas encore d'évaluation
- ITT270 Task3 RCS1103CDocument5 pagesITT270 Task3 RCS1103CAdib AfhamPas encore d'évaluation
- Experiment 7Document3 pagesExperiment 7AAAAALLENNPas encore d'évaluation
- Form Surveilans April 2017 - MutiaDocument6 pagesForm Surveilans April 2017 - MutiaUmmu TazkiyatunnafsiPas encore d'évaluation
- Laboratory Hygiene and SafetyDocument34 pagesLaboratory Hygiene and SafetyResmiPas encore d'évaluation
- Prepared By: Ulfat Amin MSC Pediatric NursingDocument25 pagesPrepared By: Ulfat Amin MSC Pediatric NursingAngelic khanPas encore d'évaluation
- Risk Assessment For Balustrade Glass InstallationDocument3 pagesRisk Assessment For Balustrade Glass InstallationNicos PapadopoulosPas encore d'évaluation
- 31congenital GlaucomasDocument12 pages31congenital GlaucomasShari' Si WahyuPas encore d'évaluation
- Kinds of Hazard and Risk ManagementDocument8 pagesKinds of Hazard and Risk ManagementShahid HussainPas encore d'évaluation
- E136Document4 pagesE136Subramanya RaoPas encore d'évaluation
- Voyeuristic Disorder SymptomsDocument7 pagesVoyeuristic Disorder SymptomsgoyaPas encore d'évaluation
- Risk for Infection AssessmentDocument7 pagesRisk for Infection AssessmentLouis RoderosPas encore d'évaluation
- OPINION ESSAY AbortionDocument2 pagesOPINION ESSAY AbortionLuisa Patiño100% (1)
- Do Your Genes Make You A CriminalDocument39 pagesDo Your Genes Make You A CriminalParisha SinghPas encore d'évaluation
- Congenital LaryngomalaciaDocument8 pagesCongenital LaryngomalaciaRettha SigiroPas encore d'évaluation
- 67166-Apvma Veterinary Medicines Technical Report TemplateDocument42 pages67166-Apvma Veterinary Medicines Technical Report Templateali aimanPas encore d'évaluation
- BDS 3rd Year Oral Pathology NotesDocument35 pagesBDS 3rd Year Oral Pathology NotesDaniyal BasitPas encore d'évaluation
- 11 - Comfort, Rest and Sleep Copy 6Document28 pages11 - Comfort, Rest and Sleep Copy 6Abdallah AlasalPas encore d'évaluation
- Alfa ArbutinDocument49 pagesAlfa ArbutinReno Vier100% (1)
- BAH Press Release (Feb. 20, 2023)Document1 pageBAH Press Release (Feb. 20, 2023)Sinclair Broadcast Group - EugenePas encore d'évaluation
- K55 MSDSDocument7 pagesK55 MSDSalocPas encore d'évaluation
- Abbott Rabeprazole PM e PDFDocument45 pagesAbbott Rabeprazole PM e PDFdonobacaPas encore d'évaluation
- Q1. Read The Passage Given Below and Answer The Questions That FollowDocument2 pagesQ1. Read The Passage Given Below and Answer The Questions That FollowUdikshaPas encore d'évaluation
- Thesis-Android-Based Health-Care Management System: July 2016Document66 pagesThesis-Android-Based Health-Care Management System: July 2016Noor Md GolamPas encore d'évaluation
- Being A Medical DoctorDocument14 pagesBeing A Medical DoctorMichael Bill GihonPas encore d'évaluation
- Incident Reports 2017-2019Document8 pagesIncident Reports 2017-2019Buddzilla FranciscoPas encore d'évaluation
- Remote Working A Dream Job British English Advanced c1 c2 GroupDocument5 pagesRemote Working A Dream Job British English Advanced c1 c2 GroupNick ManishevPas encore d'évaluation
- Wirmen Beautycare Cloth Pad SDN - BHDDocument9 pagesWirmen Beautycare Cloth Pad SDN - BHDadilahPas encore d'évaluation