Vous aimerez peut-être aussi
- Blood Banking and Transfusion Medicine Practice QuestionsDocument45 pagesBlood Banking and Transfusion Medicine Practice QuestionsVincent Reyes85% (40)
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtD'EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtÉvaluation : 5 sur 5 étoiles5/5 (1)
- 7 - Nursing Service Floating and Pull OutDocument4 pages7 - Nursing Service Floating and Pull Outakositabon100% (3)
- Valvular Heart Disease Medical Surgical NursingDocument75 pagesValvular Heart Disease Medical Surgical NursingGodfrey Franco88% (8)
- Valvular Heart DiseaseDocument54 pagesValvular Heart DiseaseRommanah AzmiPas encore d'évaluation
- Heart BlockDocument26 pagesHeart BlockMihir Patel86% (7)
- HESI Study Guide Psychiatric NursingDocument26 pagesHESI Study Guide Psychiatric NursingDean Winchester100% (4)
- Inflammatory and Valvular DisordersDocument43 pagesInflammatory and Valvular DisordersRifqi Hary ZulfikarPas encore d'évaluation
- Valvular Heart DiseaseDocument73 pagesValvular Heart Diseaseindia2puppy100% (4)
- ACFrOgC-pzE5RQJIbCELZhV0cdk6ioDNIaJcmCjwqiRF DrvgVB6DZwpe H0xKtsQ-azwWzcoEmilNTpD-bIlbSmB5BUuUaB1XyQtaHmg4Ko6DsOFWTXCUb6HV9ROfpC cuspVp0vX5MLV8nPIBCDocument67 pagesACFrOgC-pzE5RQJIbCELZhV0cdk6ioDNIaJcmCjwqiRF DrvgVB6DZwpe H0xKtsQ-azwWzcoEmilNTpD-bIlbSmB5BUuUaB1XyQtaHmg4Ko6DsOFWTXCUb6HV9ROfpC cuspVp0vX5MLV8nPIBCClaire GidoPas encore d'évaluation
- VHD: Types, Causes, Symptoms & ManagementDocument42 pagesVHD: Types, Causes, Symptoms & ManagementareeparambilPas encore d'évaluation
- Valvular Heart Disease. KulDocument67 pagesValvular Heart Disease. KulDebyAntatifaniRitongaPas encore d'évaluation
- Cardiovascular Function: Marquez, Spencer T. BSN Iii, Block Iv NCM 114, N134Document38 pagesCardiovascular Function: Marquez, Spencer T. BSN Iii, Block Iv NCM 114, N134hayascent hilarioPas encore d'évaluation
- Cardio HaikuDocument84 pagesCardio HaikugarifoPas encore d'évaluation
- Valvular Disorders: Reported By: Charlene Dorothy S. TabigneDocument34 pagesValvular Disorders: Reported By: Charlene Dorothy S. TabigneCharlene TabignePas encore d'évaluation
- Valvular Heart Disease Nursing Care and DiagnosisDocument41 pagesValvular Heart Disease Nursing Care and DiagnosisVirendra Shekhawat100% (1)
- 3 - Valvular Heart DiseasesDocument31 pages3 - Valvular Heart DiseasesLobna ElkilanyPas encore d'évaluation
- MITRAL STENOSIS AND AORTIC STENOSIS CAUSES, SYMPTOMS AND TREATMENTDocument6 pagesMITRAL STENOSIS AND AORTIC STENOSIS CAUSES, SYMPTOMS AND TREATMENTKobby AmoahPas encore d'évaluation
- Rheumatic Heart DiseaseDocument35 pagesRheumatic Heart DiseaseSAYMABANUPas encore d'évaluation
- Heart FailureDocument39 pagesHeart FailureMuhammad AsifPas encore d'évaluation
- Mitral Stenosis Facts, Causes, Symptoms and TreatmentDocument16 pagesMitral Stenosis Facts, Causes, Symptoms and TreatmentAsrafur RahmanPas encore d'évaluation
- SH - Structural, Infectious, Inflammatory Cardiac Disorders and Severe Complications of Heart Disease2014Document150 pagesSH - Structural, Infectious, Inflammatory Cardiac Disorders and Severe Complications of Heart Disease2014Jay VillasotoPas encore d'évaluation
- Lecture 17a VHDDocument70 pagesLecture 17a VHDKishan ArrumugamPas encore d'évaluation
- Cardio Vascular DisordersDocument62 pagesCardio Vascular DisordersUday Kumar100% (1)
- 6. Митральные пороки. Клиника, диагностика, лечениеDocument42 pages6. Митральные пороки. Клиника, диагностика, лечениеabarna abiPas encore d'évaluation
- Cardiac Heart Failure Guide: Causes, Symptoms & Nursing CareDocument43 pagesCardiac Heart Failure Guide: Causes, Symptoms & Nursing CareCindy DeliaPas encore d'évaluation
- Valvular Heart Disease GuideDocument43 pagesValvular Heart Disease Guideurmila prajapatiPas encore d'évaluation
- Heart Failure and Pulmonary EdemaDocument60 pagesHeart Failure and Pulmonary EdemaYosra —Pas encore d'évaluation
- Angelina A Joho MSC in Critical Care and TraumaDocument50 pagesAngelina A Joho MSC in Critical Care and TraumaZabron LuhendePas encore d'évaluation
- Congenital Heart Disease: Thoracic Conference Frank Nami, M.DDocument49 pagesCongenital Heart Disease: Thoracic Conference Frank Nami, M.DMarie CrystallinePas encore d'évaluation
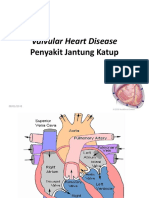
- Valvular Heart Disease: Penyakit Jantung KatupDocument40 pagesValvular Heart Disease: Penyakit Jantung KatupinhaPas encore d'évaluation
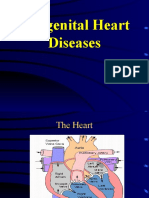
- Congenital Heart DiseaseDocument38 pagesCongenital Heart DiseaseSnIP StandredPas encore d'évaluation
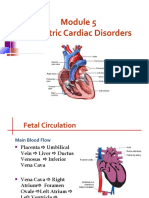
- Pediatric Cardiac Disorders: Fetal Circulation and Congestive Heart FailureDocument62 pagesPediatric Cardiac Disorders: Fetal Circulation and Congestive Heart FailureMarie Queenly Pagaran100% (1)
- Valvular Heart Defects and Infective Endocarditis-3Document37 pagesValvular Heart Defects and Infective Endocarditis-3nicholasacquah680Pas encore d'évaluation
- Valvular Heart DiseaseDocument55 pagesValvular Heart Diseaseapi-19916399Pas encore d'évaluation
- 4 - (CHF), IschemicDocument31 pages4 - (CHF), IschemicLobna ElkilanyPas encore d'évaluation
- 3 - Valvular Heart DiseasesDocument43 pages3 - Valvular Heart DiseasesHamzehPas encore d'évaluation
- K7 - Penyakit Jantung Katub-ANNDocument38 pagesK7 - Penyakit Jantung Katub-ANNXeniel AlastairPas encore d'évaluation
- Dr. Musnidarti, SPJP, FihaDocument72 pagesDr. Musnidarti, SPJP, FihasovianPas encore d'évaluation
- Valvular Heart DiseaseDocument66 pagesValvular Heart DiseaseRita LakhaniPas encore d'évaluation
- Valvular heart disease diagnosis and treatmentDocument38 pagesValvular heart disease diagnosis and treatmentDumora FatmaPas encore d'évaluation
- 1 - CHDDocument41 pages1 - CHDأمـل .Pas encore d'évaluation
- Valvular Heart DiseaseDocument5 pagesValvular Heart DiseaseElyas MehdarPas encore d'évaluation
- Aortic RegurgitationDocument3 pagesAortic RegurgitationKhalid Mahmud Arifin100% (1)
- 25) Aetiology and Pathogenesis of Valvular Heart DiseaseDocument34 pages25) Aetiology and Pathogenesis of Valvular Heart DiseaseGurrajvin Singh0% (1)
- Valvular Heart Diseases: Causes, Symptoms, and TreatmentDocument32 pagesValvular Heart Diseases: Causes, Symptoms, and TreatmentChrystel Mae PañaresPas encore d'évaluation
- Valvular Heart DiseaseDocument25 pagesValvular Heart DiseaseRyan VachaparampilPas encore d'évaluation
- Types and Management of Valvular Heart DiseaseDocument60 pagesTypes and Management of Valvular Heart DiseaseIntan Kumalasari RambePas encore d'évaluation
- Congestive Heart FailureDocument25 pagesCongestive Heart FailuredevianiamalinaPas encore d'évaluation
- Congenital Heart Disease: PathophysiologyDocument21 pagesCongenital Heart Disease: PathophysiologyChin Chan100% (1)
- 3 Three - Mitral RegurgeDocument23 pages3 Three - Mitral Regurgeمحمد بن الصادقPas encore d'évaluation
- Valvularheart Diseases: PathophysiologyDocument9 pagesValvularheart Diseases: PathophysiologyVoid LessPas encore d'évaluation
- 4 Valvular Heart Disease ICMPD (Autosaved)Document30 pages4 Valvular Heart Disease ICMPD (Autosaved)mus zaharaPas encore d'évaluation
- Cardio My Opa ThiesDocument73 pagesCardio My Opa Thiesriyazadsumaiyajb2003Pas encore d'évaluation
- Curs 9 Myocarditis CardiomyopathyDocument41 pagesCurs 9 Myocarditis CardiomyopathyIliescu DenisaPas encore d'évaluation
- Congenital Cardiac DiseaseDocument49 pagesCongenital Cardiac Diseasethapan87Pas encore d'évaluation
- ucu-CHDs_240114_230618 (2)Document68 pagesucu-CHDs_240114_230618 (2)BrianPas encore d'évaluation
- Cardiac Tamponade: Mrs. D.Melba Sahaya Sweety.D M.SC Nursing GimsarDocument23 pagesCardiac Tamponade: Mrs. D.Melba Sahaya Sweety.D M.SC Nursing GimsarD. Melba S.S ChinnaPas encore d'évaluation
- Heart Failure GuideDocument8 pagesHeart Failure GuideAikoP.NarcisoPas encore d'évaluation
- Valvular Heart DiseasesDocument60 pagesValvular Heart DiseasesEthiopia TekdemPas encore d'évaluation
- Understanding Cyanotic Heart DefectsDocument88 pagesUnderstanding Cyanotic Heart DefectsleenaPas encore d'évaluation
- Types Heart Failure PDFDocument10 pagesTypes Heart Failure PDFHannaPas encore d'évaluation
- 23 May 2011 Peerapat Thaisiam Yossavadee RuamcharoenDocument109 pages23 May 2011 Peerapat Thaisiam Yossavadee RuamcharoenRapid MedicinePas encore d'évaluation
- Heart Valve DiseaseDocument67 pagesHeart Valve DiseaseSaba SivaPas encore d'évaluation
- Unit - 1 The Cells, Tissues and Organisation of The BodyDocument36 pagesUnit - 1 The Cells, Tissues and Organisation of The BodyMihir PatelPas encore d'évaluation
- Drowning and PoisoningDocument26 pagesDrowning and PoisoningMihir PatelPas encore d'évaluation
- Unit - 1 The Cells, Tissues and Organisation of The BodyDocument36 pagesUnit - 1 The Cells, Tissues and Organisation of The BodyMihir PatelPas encore d'évaluation
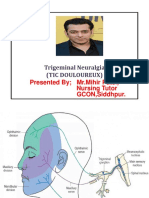
- Trigeminal NeuralgiaDocument15 pagesTrigeminal NeuralgiaMihir Patel75% (4)
- PeritonitisDocument11 pagesPeritonitisMihir PatelPas encore d'évaluation
- PancreatitisDocument18 pagesPancreatitisMihir PatelPas encore d'évaluation
- Pulmonary TuberculosisDocument12 pagesPulmonary TuberculosisMihir PatelPas encore d'évaluation
- RENBUT BHN LAB 2022 SD Agt 2023Document3 pagesRENBUT BHN LAB 2022 SD Agt 2023ajisPas encore d'évaluation
- Cosmetic Chemistry - Introduction 1Document10 pagesCosmetic Chemistry - Introduction 1Akshaya KBPas encore d'évaluation
- Microorganism staining techniques explainedDocument5 pagesMicroorganism staining techniques explainednadiazkiPas encore d'évaluation
- Respiratory Acidosis: Prepared By: Riezel Umaming Kathleen Testado Hazel AlarillaDocument16 pagesRespiratory Acidosis: Prepared By: Riezel Umaming Kathleen Testado Hazel AlarillaDareRaymond100% (2)
- Attesta™ DR Mri Surescan™ Atdr01: Dual Chamber Rate Responsive Pacemaker (DDDR)Document42 pagesAttesta™ DR Mri Surescan™ Atdr01: Dual Chamber Rate Responsive Pacemaker (DDDR)mytake100Pas encore d'évaluation
- Chapter 27 - Anxiety-Related, Obsessive-Compulsive, Trauma and Stressor-Related, Somatic, and Dissociative DisordersDocument10 pagesChapter 27 - Anxiety-Related, Obsessive-Compulsive, Trauma and Stressor-Related, Somatic, and Dissociative DisordersKTPas encore d'évaluation
- Minimally Invasive Spine SurgeryDocument510 pagesMinimally Invasive Spine SurgeryLuis RodriguezPas encore d'évaluation
- Hormonal Replacement Therapy Lesson PlanDocument9 pagesHormonal Replacement Therapy Lesson PlanBaljinder kaurPas encore d'évaluation
- CholesteatomaDocument44 pagesCholesteatomavna297Pas encore d'évaluation
- Primary Chest Wall Hydatid Cyst - A Rare Case Report: - PresenterDocument8 pagesPrimary Chest Wall Hydatid Cyst - A Rare Case Report: - PresenterEdison Varghese VadakkencheryPas encore d'évaluation
- Group 1 Case Study Chapter 24Document10 pagesGroup 1 Case Study Chapter 24Doneva Lyn MedinaPas encore d'évaluation
- Maternal & Child Care Nursing Table of ContentsDocument2 pagesMaternal & Child Care Nursing Table of Contentsɹǝʍdןnos100% (4)
- Presented by DR Rahul D AgrawalDocument64 pagesPresented by DR Rahul D AgrawalRahul AgrawalPas encore d'évaluation
- Implant Failure and ManagementDocument59 pagesImplant Failure and ManagementDrIbrahimShaikh0% (1)
- Sop For Thalassemia Screening Wwith NbsDocument11 pagesSop For Thalassemia Screening Wwith NbsUMMID WashimPas encore d'évaluation
- MOH, DHA and HAAD recalls from 2017 WhatsApp groupDocument32 pagesMOH, DHA and HAAD recalls from 2017 WhatsApp groupshahzadPas encore d'évaluation
- Use of Local and Axial Pattern Flaps For Reconstruction of The Hard and Soft Palate PDFDocument9 pagesUse of Local and Axial Pattern Flaps For Reconstruction of The Hard and Soft Palate PDFJose Luis Granados SolerPas encore d'évaluation
- Vital Signs ChecklistDocument21 pagesVital Signs ChecklistJapsay Francisco GranadaPas encore d'évaluation
- Thyroid StormDocument3 pagesThyroid StormSuprit SnPas encore d'évaluation
- Adverse Reaction Blood BankDocument10 pagesAdverse Reaction Blood BankyourfamilydoctorPas encore d'évaluation
- Thyroid Diseases in Pregnancy PMK HandoutDocument12 pagesThyroid Diseases in Pregnancy PMK HandoutWikrom Keng WromKiPas encore d'évaluation
- For The Best Sinus Congestion RemediesDocument4 pagesFor The Best Sinus Congestion Remedies4zaleakuPas encore d'évaluation
- KEILMUAN DAN SENI DALM KEBIDANANDocument18 pagesKEILMUAN DAN SENI DALM KEBIDANANRizky Putri AndriantiPas encore d'évaluation
- Nursing Care of a Patient with Hypovolemic ShockDocument46 pagesNursing Care of a Patient with Hypovolemic ShockBianca MaePas encore d'évaluation
- Eclampsia Guidelines FINAL Ratified MCYP SG Sept20 15Document20 pagesEclampsia Guidelines FINAL Ratified MCYP SG Sept20 15Grigore PopaPas encore d'évaluation
- Hematology - Oncology - PREP 2021Document46 pagesHematology - Oncology - PREP 2021drthanalla100% (1)
- Clinical Practice Guidelines For Rest OrthosisDocument8 pagesClinical Practice Guidelines For Rest OrthosisJavier HonoldPas encore d'évaluation