Vous aimerez peut-être aussi
- Davis Med Notes2Document242 pagesDavis Med Notes2Yucef Bahian-AbangPas encore d'évaluation
- Medication Fact Book for Psychiatric Practice, Fifth EditionD'EverandMedication Fact Book for Psychiatric Practice, Fifth EditionPas encore d'évaluation
- Rehabilitation of Muscle Dysfunction in HemophiliaDocument14 pagesRehabilitation of Muscle Dysfunction in HemophiliadavidcorzoPas encore d'évaluation
- Ed enDocument376 pagesEd enNashria Rusdhy100% (2)
- Modalities and Physical Agents For The Rehab ProfessionalDocument6 pagesModalities and Physical Agents For The Rehab ProfessionalJyrra NeriPas encore d'évaluation
- Drug CompilationDocument39 pagesDrug CompilationANa AntonioPas encore d'évaluation
- Running Head: Occupational Profile and Intervention Plan 1Document19 pagesRunning Head: Occupational Profile and Intervention Plan 1api-292735638Pas encore d'évaluation
- Essensial DrugDocument363 pagesEssensial Drugwilliam28asshole100% (1)
- Fibroid & Cyst ProtocolDocument32 pagesFibroid & Cyst ProtocolTheresa DalePas encore d'évaluation
- Gabapentin Oi DesDocument11 pagesGabapentin Oi DesLuis Felipe Arteaga ArredondoPas encore d'évaluation
- Essay Plans For GAMSATDocument11 pagesEssay Plans For GAMSATrosh100% (1)
- Complementary and Alternative Medicine (CAM) Supplement Use in People with Diabetes: A Clinician's Guide: A Clinician's GuideD'EverandComplementary and Alternative Medicine (CAM) Supplement Use in People with Diabetes: A Clinician's Guide: A Clinician's GuidePas encore d'évaluation
- Viva 1Document500 pagesViva 1Jan Jansen67% (3)
- PH Info ExamDocument44 pagesPH Info ExamANa AntonioPas encore d'évaluation
- Pain As 5th Vital SignDocument70 pagesPain As 5th Vital SignPoornima GopalPas encore d'évaluation
- PRACTICITIONER Reference To Nieper SupplementsDocument95 pagesPRACTICITIONER Reference To Nieper SupplementsClóvis Valadares100% (1)
- Reflection Report Sulam Project Muhamad Akmal Bin AzmanDocument14 pagesReflection Report Sulam Project Muhamad Akmal Bin AzmanmPas encore d'évaluation
- The Surgical Team: Intraoperative NursingDocument4 pagesThe Surgical Team: Intraoperative NursingGiselle Chloe Baluya icoPas encore d'évaluation
- Alleviating The Access Abyss in Palliative Care and Pain Relief: An Imperative of Universal Health CoverageDocument36 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief: An Imperative of Universal Health CoveragePresentaciones_FKPas encore d'évaluation
- Product Monograph: WWW - Pfizer.caDocument29 pagesProduct Monograph: WWW - Pfizer.caAndre UrsescuPas encore d'évaluation
- Mirtazapine Toxicity in CatsDocument7 pagesMirtazapine Toxicity in CatsAllana Valau MoreiraPas encore d'évaluation
- Scientific Discussion - En.idDocument9 pagesScientific Discussion - En.idassajadda lizikriPas encore d'évaluation
- Nitrosamine Impurities - Current Status and Expectations: Dr. Milind JoshiDocument31 pagesNitrosamine Impurities - Current Status and Expectations: Dr. Milind JoshihuykhiemPas encore d'évaluation
- Methylphenidate March 2018 RevisedDocument14 pagesMethylphenidate March 2018 RevisedEmotional EternalPas encore d'évaluation
- Drug Profile Comparison Between PitolisantDocument3 pagesDrug Profile Comparison Between Pitolisantakshay dahiwelePas encore d'évaluation
- Keppra DueDocument4 pagesKeppra Dueapi-734449276Pas encore d'évaluation
- Duragesic Mat PM eDocument46 pagesDuragesic Mat PM ePSmPas encore d'évaluation
- 2010 Bandelow ExtendedDocument16 pages2010 Bandelow ExtendedRian YupitaPas encore d'évaluation
- Guidance On The Rational Use of RH Kit 3 (Post Rape Management)Document8 pagesGuidance On The Rational Use of RH Kit 3 (Post Rape Management)hiba.khellowPas encore d'évaluation
- Amfetamine OverdoseDocument52 pagesAmfetamine Overdosemanuel ricardo barojas alvarezPas encore d'évaluation
- Slides - Product - DR Chen - 100320 - 2010 - Road+Show - E (Rev 03)Document30 pagesSlides - Product - DR Chen - 100320 - 2010 - Road+Show - E (Rev 03)Kogree Kyaw Win Oo100% (1)
- Shin LuluDocument2 pagesShin LuluEka HimawanPas encore d'évaluation
- Pharmaco Vigilance of ASU Drugs:an Over View of Current Status, Challenges and SolutionsDocument55 pagesPharmaco Vigilance of ASU Drugs:an Over View of Current Status, Challenges and Solutionssuhas M100% (1)
- Mixtard Epar Summary Public - enDocument3 pagesMixtard Epar Summary Public - enPES 2022Pas encore d'évaluation
- Valproate For Agitation in Critically Ill Patients - A Retrospective Study-2017Document7 pagesValproate For Agitation in Critically Ill Patients - A Retrospective Study-2017Juan ParedesPas encore d'évaluation
- Regimen Dose of SimvastatinDocument14 pagesRegimen Dose of Simvastatinmuhammad thohaPas encore d'évaluation
- Gabapentina y Mirtazapina Post-OvarioDocument8 pagesGabapentina y Mirtazapina Post-OvarioPaola Almengor PinedoPas encore d'évaluation
- Diabetic Neuropathy RCT (Diacon 2017)Document17 pagesDiabetic Neuropathy RCT (Diacon 2017)Prof. Dr. Manishkumar PatelPas encore d'évaluation
- Lyrica PM E 237599 2020.05.11Document62 pagesLyrica PM E 237599 2020.05.11qa officerPas encore d'évaluation
- Comparative e Cacy and Acceptability of Antimanic Drugs in Acute Mania: A Multiple-Treatments Meta-AnalysisDocument10 pagesComparative e Cacy and Acceptability of Antimanic Drugs in Acute Mania: A Multiple-Treatments Meta-AnalysisCarolina PradoPas encore d'évaluation
- Adalat XL PM Eng - 0Document35 pagesAdalat XL PM Eng - 0Geo GeoPas encore d'évaluation
- Prodi: Profesi Apoteker 37 / Kelas A Judul Jurnal: Drug Use Evaluation of Three Widely Prescribed Antibiotics in ADocument2 pagesProdi: Profesi Apoteker 37 / Kelas A Judul Jurnal: Drug Use Evaluation of Three Widely Prescribed Antibiotics in AZhafirah BojonegoroPas encore d'évaluation
- Epo PrintDocument2 pagesEpo Printpebriana dian ePas encore d'évaluation
- KB HormonalDocument65 pagesKB Hormonaljessica_siahaan_1Pas encore d'évaluation
- Proposal For The Inclusion of Anti-Emetic Medications (For Children) in The Who Model List of Essential MedicinesDocument44 pagesProposal For The Inclusion of Anti-Emetic Medications (For Children) in The Who Model List of Essential MedicinesJennifer FaustinPas encore d'évaluation
- Analgesia Guidelines PaediatricDocument23 pagesAnalgesia Guidelines PaediatricsyahmiPas encore d'évaluation
- Acep Equal Opiod Wave IiDocument43 pagesAcep Equal Opiod Wave IiJesse M. MassiePas encore d'évaluation
- Handout 2563 OpioidsDocument84 pagesHandout 2563 OpioidsPiya TangPas encore d'évaluation
- Dr. Lisa Marsch's NPF PresentationDocument32 pagesDr. Lisa Marsch's NPF PresentationNational Press Foundation100% (1)
- Hot Topics in Internal MedicineDocument9 pagesHot Topics in Internal Medicinekhangsiean89Pas encore d'évaluation
- Pharma - FinalsDocument6 pagesPharma - Finalsannie lalangPas encore d'évaluation
- Medicines Administration 1 Understanding Routes of AdministrationDocument3 pagesMedicines Administration 1 Understanding Routes of AdministrationJosa Camille BungayPas encore d'évaluation
- Changes Include Addition of Nattokinase As First Line Therapy and Reordering of First-And Second-Line TherapiesDocument60 pagesChanges Include Addition of Nattokinase As First Line Therapy and Reordering of First-And Second-Line TherapiesJoshua VanhiePas encore d'évaluation
- WHO - Essential Drugs PDFDocument376 pagesWHO - Essential Drugs PDFnrhmhealthPas encore d'évaluation
- Bioav 3Document264 pagesBioav 3Sabiruddin Mirza DipuPas encore d'évaluation
- Diabetic Peripheral Neuropathy Enhanced Primary Care Pathway FINAL Feb 7 2018 For PostingDocument4 pagesDiabetic Peripheral Neuropathy Enhanced Primary Care Pathway FINAL Feb 7 2018 For PostingNurul FajriPas encore d'évaluation
- Management of Poisoning - Booklet PDFDocument344 pagesManagement of Poisoning - Booklet PDFkrysteenPas encore d'évaluation
- Repaglinide LDocument19 pagesRepaglinide LbigbullsrjPas encore d'évaluation
- An Off-Label Guide To Gabapentin 2022-01-31 CARLAT PUBLISHINGDocument1 pageAn Off-Label Guide To Gabapentin 2022-01-31 CARLAT PUBLISHINGLee ThompsonPas encore d'évaluation
- ED enDocument363 pagesED enMunsif Ali100% (1)
- DrugDocument363 pagesDruglakjdsflfdskj100% (1)
- Essential Drug - User GuideDocument363 pagesEssential Drug - User Guideakramuddaula100% (1)
- Cara Pakai ObatDocument362 pagesCara Pakai ObatEddy Adnyana100% (1)
- Essential Drugs enDocument363 pagesEssential Drugs enDunca Ana-MariaPas encore d'évaluation
- Migraine A Summary of Existing Guidelines For UseDocument9 pagesMigraine A Summary of Existing Guidelines For UseHajrah SuhardiPas encore d'évaluation
- Critical Care SedationD'EverandCritical Care SedationAngelo Raffaele De GaudioPas encore d'évaluation
- Innovations in Breast Cancer TreatmentDocument21 pagesInnovations in Breast Cancer TreatmentPresentaciones_FKPas encore d'évaluation
- Closing The Cancer Divide & Strengthening Health Systems: Interwoven OpportunitiesDocument39 pagesClosing The Cancer Divide & Strengthening Health Systems: Interwoven OpportunitiesPresentaciones_FKPas encore d'évaluation
- Closing Cancer Divided: Expanding Access To Care & ControlDocument46 pagesClosing Cancer Divided: Expanding Access To Care & ControlPresentaciones_FKPas encore d'évaluation
- La Mujer Ante El COVID-19: Retos y Oportunidades para La Salud y El Sector Salud.Document36 pagesLa Mujer Ante El COVID-19: Retos y Oportunidades para La Salud y El Sector Salud.Presentaciones_FKPas encore d'évaluation
- The Health and Caregiving Workforce: An Array of InequitiesDocument16 pagesThe Health and Caregiving Workforce: An Array of InequitiesPresentaciones_FKPas encore d'évaluation
- Closing The Global Pain Divide: An Equity and Health ImperativeDocument16 pagesClosing The Global Pain Divide: An Equity and Health ImperativePresentaciones_FKPas encore d'évaluation
- Unpaid Health Care and Caregiving: A Gendered and Hidden Yet Indispensable Subsidy To Economic and Social Development.Document16 pagesUnpaid Health Care and Caregiving: A Gendered and Hidden Yet Indispensable Subsidy To Economic and Social Development.Presentaciones_FKPas encore d'évaluation
- Breast Cancer Disparities: Closing Global DividesDocument37 pagesBreast Cancer Disparities: Closing Global DividesPresentaciones_FKPas encore d'évaluation
- Breast Cancer in The Americas: Closing Divides Through Systemic Innovation & AdvocacyDocument33 pagesBreast Cancer in The Americas: Closing Divides Through Systemic Innovation & AdvocacyPresentaciones_FKPas encore d'évaluation
- Closing The Divide in Access To Palliative Care and Pain ReliefDocument45 pagesClosing The Divide in Access To Palliative Care and Pain ReliefPresentaciones_FKPas encore d'évaluation
- Breast Cancer in The AmericasDocument27 pagesBreast Cancer in The AmericasPresentaciones_FKPas encore d'évaluation
- Alleviating The Access Abyss in Palliative Care and Pain Relief.Document37 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief.Presentaciones_FKPas encore d'évaluation
- Alleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoverageDocument19 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoveragePresentaciones_FKPas encore d'évaluation
- Alleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoverageDocument18 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoveragePresentaciones_FKPas encore d'évaluation
- Closing The Cancer DivideDocument36 pagesClosing The Cancer DividePresentaciones_FKPas encore d'évaluation
- Alleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoverageDocument44 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoveragePresentaciones_FKPas encore d'évaluation
- Closing The Cancer Divide For Women in The Americas: Diagonal Health System InnovationsDocument39 pagesClosing The Cancer Divide For Women in The Americas: Diagonal Health System InnovationsPresentaciones_FKPas encore d'évaluation
- Evidence-Inspired Advocacy and Advocacy-Based EvidenceDocument35 pagesEvidence-Inspired Advocacy and Advocacy-Based EvidencePresentaciones_FKPas encore d'évaluation
- Closing Cancer Divided: Expanding Access To Care & ControlDocument41 pagesClosing Cancer Divided: Expanding Access To Care & ControlPresentaciones_FKPas encore d'évaluation
- Closing The Cancer Divide: Lessons From Women's HealthDocument43 pagesClosing The Cancer Divide: Lessons From Women's HealthPresentaciones_FKPas encore d'évaluation
- Closing Divides To Meet The Challenge of Women S CancerDocument22 pagesClosing Divides To Meet The Challenge of Women S CancerPresentaciones_FKPas encore d'évaluation
- Health System Responses To Women's Cancers in The AmericasDocument36 pagesHealth System Responses To Women's Cancers in The AmericasPresentaciones_FKPas encore d'évaluation
- Closing The Cancer Divide: Challenges and OpportunitiesDocument51 pagesClosing The Cancer Divide: Challenges and OpportunitiesPresentaciones_FKPas encore d'évaluation
- Reducing The Cancer Divide For Breast and Cervical CancerDocument53 pagesReducing The Cancer Divide For Breast and Cervical CancerPresentaciones_FKPas encore d'évaluation
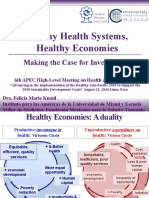
- Healthy Health Systems, Healthy Economies. Making The Case For Investment.Document28 pagesHealthy Health Systems, Healthy Economies. Making The Case For Investment.Presentaciones_FKPas encore d'évaluation
- Women's Cancers in The Americas: Closing DividesDocument35 pagesWomen's Cancers in The Americas: Closing DividesPresentaciones_FKPas encore d'évaluation
- Evidence-Inspired Advocacy and Advocacy-Based EvidenceDocument35 pagesEvidence-Inspired Advocacy and Advocacy-Based EvidencePresentaciones_FKPas encore d'évaluation
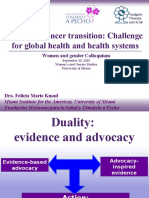
- Women's Cancer Transition: Challenge For Global Health and Health SystemsDocument58 pagesWomen's Cancer Transition: Challenge For Global Health and Health SystemsPresentaciones_FKPas encore d'évaluation
- NCPDocument14 pagesNCPRaidis Pangilinan0% (1)
- Applying The Biopsychosocial Model To The Management of Rheumatic Disease PDFDocument14 pagesApplying The Biopsychosocial Model To The Management of Rheumatic Disease PDFlumi_vulpitzaPas encore d'évaluation
- 9 Laporan Pasien UmumDocument222 pages9 Laporan Pasien UmumANDRES PULANA 521201018Pas encore d'évaluation
- Daftar Pustaka HNPDocument11 pagesDaftar Pustaka HNPYusnaedi DidiPas encore d'évaluation
- Askep Basing VarikokelDocument3 pagesAskep Basing VarikokelToro PutraPas encore d'évaluation
- Epidural Analgesia in LaborDocument4 pagesEpidural Analgesia in LaborVishal PrabhuPas encore d'évaluation
- Clear My Choice: Not Yet Answered Marked Out of 1.00Document34 pagesClear My Choice: Not Yet Answered Marked Out of 1.00mark OrpillaPas encore d'évaluation
- Palliative Care Lecture 2022Document20 pagesPalliative Care Lecture 2022Shreyas WalvekarPas encore d'évaluation
- CPSA Hearing Tribunal Decision - Dr. Gaylord WardellDocument27 pagesCPSA Hearing Tribunal Decision - Dr. Gaylord WardellCTV CalgaryPas encore d'évaluation
- Hypnosis and Cingulate-Mediated Mechanisms of AnalgesiaDocument20 pagesHypnosis and Cingulate-Mediated Mechanisms of AnalgesiaCristian GondacPas encore d'évaluation
- Photobiomodulation Implications For Anesthesia and Pain Relief 2016Document12 pagesPhotobiomodulation Implications For Anesthesia and Pain Relief 2016rogerPas encore d'évaluation
- Rle NotesDocument7 pagesRle NotesLorens Troy SoltisPas encore d'évaluation
- Escoja El Problema de Salud en Cada SituaciónDocument3 pagesEscoja El Problema de Salud en Cada SituaciónAlejandra OsorioPas encore d'évaluation
- Interferential Therapy 2021Document13 pagesInterferential Therapy 2021Mộng HoàngPas encore d'évaluation
- Jospt 2018 0603Document5 pagesJospt 2018 0603Chris WongPas encore d'évaluation
- Part 6 Text Hell Heaven ConclusionDocument6 pagesPart 6 Text Hell Heaven Conclusionapi-295492945Pas encore d'évaluation
- A Historical Review of Acupuncture To The Achilles TendonDocument10 pagesA Historical Review of Acupuncture To The Achilles TendonCrystal SalasPas encore d'évaluation
- JOYCE TRAVELBEE and DOROTHY JOHNSONDocument5 pagesJOYCE TRAVELBEE and DOROTHY JOHNSONRaya MesiasPas encore d'évaluation
- Drug StudyDocument3 pagesDrug StudyMa. Andrea B. PALOMOPas encore d'évaluation
- It An To: With Ina With orDocument1 pageIt An To: With Ina With orShyra MustakimPas encore d'évaluation
- Focus Charting at North Bay General Hospital DAEDocument67 pagesFocus Charting at North Bay General Hospital DAECzarina GuintoPas encore d'évaluation